Session Information
Date: Tuesday, November 10, 2015
Title: Fibromyalgia, Soft Tissue Disorders, Regional and Specific Clinical Pain Syndromes Poster II
Session Type: ACR Poster Session C
Session Time: 9:00AM-11:00AM
Background/Purpose:
Subacromial bursitis is caused by inflammation of the bursa that
separates the superior surface of the supraspinatus tendon from the overlying coraco-acromial ligament and acromion. While intra-bursal corticosteroid injection is
routinely used to treat pain and help restore function in subacromial bursitis,
the optimal corticosteroid dose or preparation is currently unknown. We hypothesized that there would be no
difference between subjects who received triamcinolone acetonide
(TAC) or methylprednisolone acetate (MP) but there would be greater improvement
with a 40 mg dose as compared to a 20 mg dose.
Methods:
This single blinded study randomized subjects with at least 2 weeks of subacromial
bursal pain by history and exam to receive intrabursal
corticosteroid in one of four groups:
TAC 20 mg, TAC 40 mg, MP 20 mg, or MP 40 mg. Concomitant with the corticosteroid injection
all subjects also received 2 mL of 1% lidocaine without epinephrine and 2 mL of
0.5% bupivacaine. The Quick Disabilities
of Arm, Shoulder, and Hand (or QuickDASH), subject reported pain, and adverse
events were recorded at time of injection and then 3 days, 3 weeks, and 6 weeks
post-injection. Primary outcome was
improvement in the QuickDASH 6 weeks post-injection. Secondary outcomes were improvement in
subject reported pain at 6 weeks and occurrence of adverse events. This trial is registered at www.clinicaltrials.gov (NCT02242630).
Results:
Forty eight subjects were recruited.
Average age was 66.8 ± 10.8 years old.
Over 85% of subjects were Caucasian.
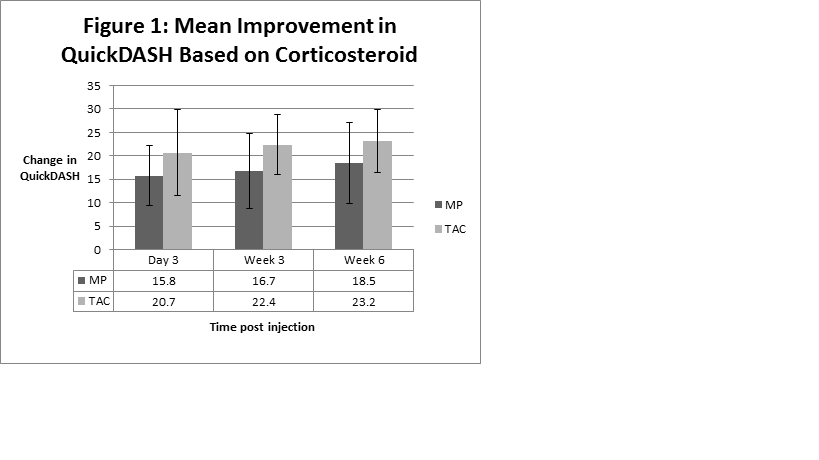
Twenty left and 28 right subacromial bursa were injected. For the primary outcome, mean improvement in
QuickDASH was similar between those who received TAC vs. MP (regardless of
dose), shown in Figure 1. Mean
improvement in QuickDASH was similar between those who received the 20 mg dose
vs. 40 mg dose (regardless of preparation), shown in Figure 2.

No
statistically significant differences in subject reported pain based on dose or
corticosteroid preparation were noted (data not shown). No statistically significant differences in
adverse events were noted between groups, although 3 subjects reported
elevations in blood glucose and 2 subjects reported diarrhea.
Conclusion:
With our modest sample size we have not identified any statistically
significant differences for subjects with subacromial bursitis treated with
either corticosteroid preparation or dose.
Subject recruitment is ongoing. No
significant trends in adverse outcomes were noted.
To cite this abstract in AMA style:
Motley S, Ramsey B, Carroll M. Improvement in Function and Pain Due to Subacromial Bursitis As Related to Dose of Triamcinolone Acetonide or Methylprednisolone Acetate [abstract]. Arthritis Rheumatol. 2015; 67 (suppl 10). https://acrabstracts.org/abstract/improvement-in-function-and-pain-due-to-subacromial-bursitis-as-related-to-dose-of-triamcinolone-acetonide-or-methylprednisolone-acetate/. Accessed .« Back to 2015 ACR/ARHP Annual Meeting
ACR Meeting Abstracts - https://acrabstracts.org/abstract/improvement-in-function-and-pain-due-to-subacromial-bursitis-as-related-to-dose-of-triamcinolone-acetonide-or-methylprednisolone-acetate/