Session Information
The 2020 Pediatric Rheumatology Symposium, originally scheduled for April 29 – May 2, was postponed due to COVID-19; therefore, abstracts were not presented as scheduled.
Date: Thursday, April 30, 2020
Title: Plenary Abstracts Session 1
Session Type: Plenary Session I
Session Time: 2:30PM-3:30PM
Background/Purpose: PRINTO recently proposed preliminary JIA classification criteria to revise the International League of Associations for Rheumatology (ILAR) criteria. The stated aim was to obtain more homogeneous groups and improve alignment with adult criteria, when appropriate. We used data from the ReACCh-Out prospective inception cohort to assess 1) the degree of reclassification that would occur with the PRINTO system, and 2) whether reclassification would improve alignment with biologically defined subtypes and adult criteria for inflammatory arthritis.
Methods: JIA patients recruited from 16 Canadian centres between January 2005–December 2010 were considered. To facilitate fair comparisons, investigators were blinded to the original physician-assigned ILAR diagnoses and patients were computationally classified to PRINTO and ILAR systems with available data. In order to improve PRINTO classification, patients were considered ANA positive with ≥1 positive ANA reading. Patients were also evaluated under criteria for 4 adult arthritides (rheumatoid arthritis, psoriatic arthritis, adult-onset Still’s disease, and spondyloarthritis). Patients who provided biological samples were assigned to one of 4 biological subtypes as previously reported [1].
ILAR and PRINTO systems were compared to each other, and to biological and adult classification systems. Relationships were visualized with Circos plots and the degree of alignment was assessed with χ2 tests.
Results: 1,238 newly diagnosed (< 7 months) JIA patients with ≥1 follow-up visit were included. According to PRINTO criteria, most patients (783, 63%) were classified as other JIA, 244 (20%) had early-onset ANA-positive JIA, 159 (13%) had enthesitis/spondylitis-related JIA, 40 (3%) had systemic JIA, 12 (1%) had RF-positive JIA, and 0 had unclassified JIA. 1,111 patients (90%) had ANA information available.
We found significant associations between ILAR and PRINTO subtypes (χ2=2,503, p< 0.001). All patients with systemic or RF-positive polyarthritis (ILAR) were categorized as systemic or RF-positive JIA (PRINTO), respectively. 136 patients (62%) with enthesitis-related arthritis (ERA, ILAR) were categorized as enthesitis/spondylitis-related (PRINTO). Other JIA included ILAR-defined oligoarthritis (n=390, 50%), RF-negative polyarthritis (178, 23%), psoriatic arthritis (54, 6.9%), ERA (81, 10%), and undifferentiated arthritis (80, 10%). In 132 patients (11%) with cytokine information, we identified associations between their biological subtypes and the ILAR system (χ2=46, p< 0.001) but not the PRINTO system (χ2=14, p=0.09) (Fig 1). Of 396 patients (32%) who satisfied adult criteria, fewer associations between the PRINTO system and adult arthritides were seen compared to the ILAR system (Fig 2, Table 1). No adult diagnosis was enriched for early-onset ANA-positive JIA.
Conclusion: Our findings suggest that adopting the preliminary PRINTO system would result in roughly two thirds of patients categorized as Other JIA and did not improve alignment with biologically defined groupings or adult classification criteria.
1. Eng SW et al. Arthritis Rheumatol. 2014; 66(12): 3463-75
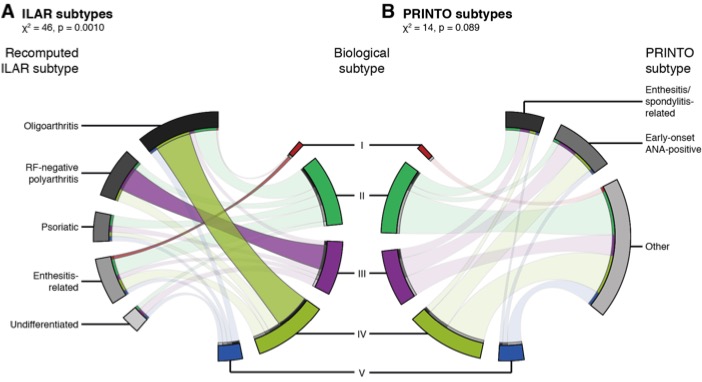
Circos figures linking patient biological phenotypes (coloured wedges; middle) with ILAR (grey wedges; left) and PRINTO categories (grey wedges; right). Ribbon widths are proportional to the number of patients between pairs of biological subtypes and ILAR or PRINTO categories. Opaquer ribbons represent pairs that are significantly associated as determined by standardized residuals from χ2 tests.
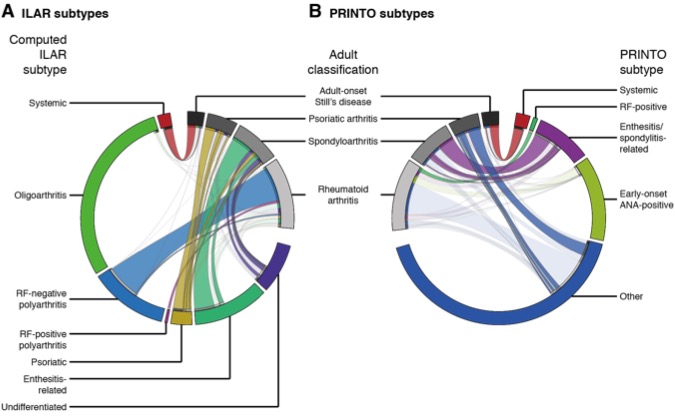
Circos figure linking computed ILAR categories (coloured wedges; left) with adult classifications (grey wedges; middle). Ribbons link patients shared between pairs of ILAR categories and adult classifications. Wider ribbons indicate more patients. Opaquer ribbons represent pairs that are significantly associated as given by standardized residuals from χ2 tests on the distributions of ILAR subtypes in each adult classification (Table 1). (B) Same as panel A, but for PRINTO categories (coloured wedges; right).
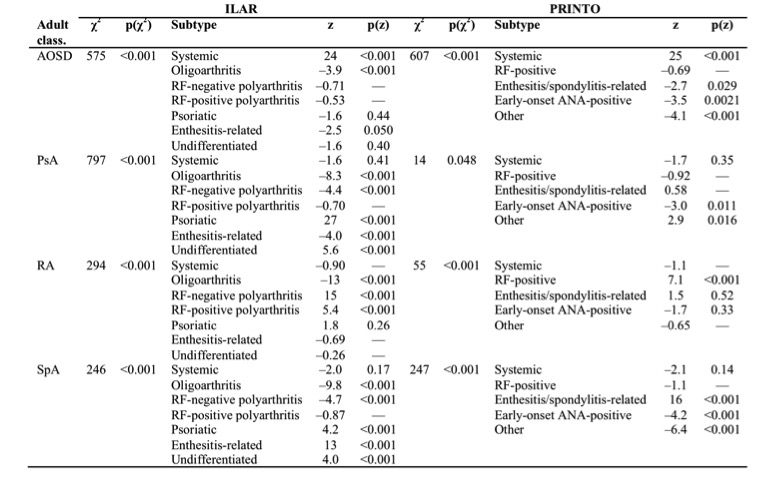
p_values were Bonferroni_adjusted to account for multiple hypothesis testing.
—, adjusted p = 1.0.
AOSD: Adult_onset Still’s Disease, PsA: Psoriatic arthritis, RA: Rheumatoid arthritis, SpA: Spondyloarthritis
To cite this abstract in AMA style:
Lee J, Eng S, Feldman B, Guzman J, Oen K, Yeung R. Implications of Adopting the Newly Proposed Pediatric Rheumatology International Trials Organization (PRINTO) Classification Criteria for Juvenile Idiopathic Arthritis (JIA): Results from the Research in Arthritis in Canadian Children, Emphasizing Outcomes (ReACCh-Out) Cohort [abstract]. Arthritis Rheumatol. 2020; 72 (suppl 4). https://acrabstracts.org/abstract/implications-of-adopting-the-newly-proposed-pediatric-rheumatology-international-trials-organization-printo-classification-criteria-for-juvenile-idiopathic-arthritis-jia-results-from-the-research/. Accessed .« Back to 2020 Pediatric Rheumatology Symposium
ACR Meeting Abstracts - https://acrabstracts.org/abstract/implications-of-adopting-the-newly-proposed-pediatric-rheumatology-international-trials-organization-printo-classification-criteria-for-juvenile-idiopathic-arthritis-jia-results-from-the-research/