Session Information
Session Type: ACR Poster Session B
Session Time: 9:00AM-11:00AM
Background/Purpose: Cardiovascular
disease (CVD) is the leading cause of death among individuals with rheumatoid
arthritis (RA). The 2010 EULAR guidelines recommend annual CV risk
assessment for all RA patients in accordance with national guidelines1.
However, CVD risks are not being assessed frequently and systematically in RA
patients. We implemented an Electronic Medical Record (EMR)-based
clinical decision support intervention at a large tertiary care center and
assessed the effects of this intervention on lipid screening among RA patients
by treating rheumatologists.
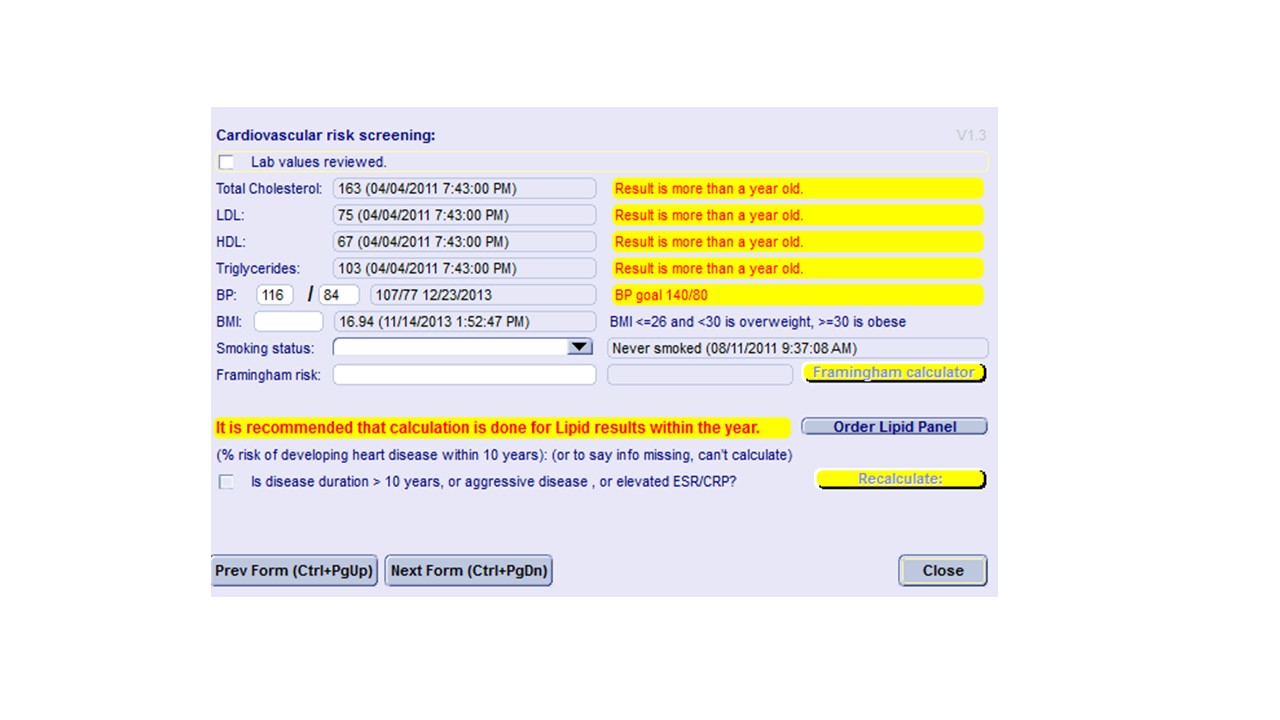
Methods: We developed a
self-populated form that was incorporated into each EMR rheumatology visit and
contained the following information (Image): 1) dates of the latest
assessment of CVD risks (body mass index (BMI), blood pressure, smoking, lipid
screening); 2) the latest values for all of the above CVD risks; 3) Framingham
risk score calculator. To evaluate the impact of this EMR-based
intervention, lipid screening rates among adult RA patients were compared pre
and post implementing this EMR tool. LDL
levels were compared for patients seen, pre-intervention, 1/1/2012-6/30/2012 (2012),
and post-intervention, 1/1/2014-6/30/2014 (2014). RA patients were
identified using a previously validated algorithm requiring two or more visits
with the ICD9 code 714.0 (Rheumatoid arthritis), and at least one
prescription for a disease modifying anti-rheumatic medication2. The
first visit within the study period was defined as the index visit.
Wilcoxon-Mann-Whitney tests were used to compare continuous variables, and
Pearson’s Chi-square tests (or Fisher’s exact test when appropriate) were used
to compare categorical variables.
Results: 131 and 111 RA
patients seen in outpatient rheumatology clinics by rheumatologists in 2012 and
2014, respectively. Sex, race, and ethnicity were similar: 35% vs. 29% were
Black, 60% and 64% were Hispanic, 12% and 9% were men.
There were no age differences: mean (SD) 58(14) years old in 2012, and 59 (14)
years old in 2014. BMI was also similar: mean (SD) 30(7) kg/m2
in 2012, and 30(6) kg/m2
in 2014. Lipid screening frequency in the subsequent 6 months was
32% in 2012 and 23% in 2014 (p=0.12). Median (SD) LDL was 96 (30) mg/dl in 2012,
and 109 (36) mg/dl in 2014 (p=0.09)
Conclusion:
Implementing an EMR based decision support tool did not improve rates of
screening for lipid abnormalities among RA patients. Lipid screening
rates remained low. Further studies are needed to identify and address
barriers to CVD screening in RA among rheumatologists and primary care
providers.
References:
1.Peters MJ, et al. Ann Rheum Dis.
2010 Feb; 69(2):325-331.
2.
Kim SY, et al. Arthritis Res Ther. 2011 Feb 23;13(1):R32)
Image:
Decision support tool to aid rheumatologists with cardiovascular screening
To cite this abstract in AMA style:
Kumthekar A, Alevizos M, Jordan N, Broder AR. Implementing an Electronic Medical Recorded-Based Clinical Decision Support Tool Did Not Improve Cardiovascular Risk Screening in Rheumatoid Arthritis Patients [abstract]. Arthritis Rheumatol. 2015; 67 (suppl 10). https://acrabstracts.org/abstract/implementing-an-electronic-medical-recorded-based-clinical-decision-support-tool-did-not-improve-cardiovascular-risk-screening-in-rheumatoid-arthritis-patients/. Accessed .« Back to 2015 ACR/ARHP Annual Meeting
ACR Meeting Abstracts - https://acrabstracts.org/abstract/implementing-an-electronic-medical-recorded-based-clinical-decision-support-tool-did-not-improve-cardiovascular-risk-screening-in-rheumatoid-arthritis-patients/