Session Information
Date: Tuesday, November 12, 2019
Title: Pediatric Rheumatology – ePoster III: Systemic JIA, Fever, & Vasculitis
Session Type: Poster Session (Tuesday)
Session Time: 9:00AM-11:00AM
Background/Purpose: Transition from pediatric to adult rheumatology care is more likely to be successful if a transition program is in place. Previously successful interventions to improve transition outcomes have included integrating an adult subspecialist in the pediatric clinic setting. We hypothesize that we will improve transition outcomes by implementing a transition clinic which includes an adult rheumatologist providing care within a pediatric rheumatology clinic.
Methods: We initiated a weekly transition clinic in November 2018 called ACCORD (Adult Center for Childhood Onset Rheumatic Disease). This clinic is staffed by 1 adult rheumatologist (board certified in internal medicine and pediatrics), 1 pediatric nurse, a research coordinator, and a social worker. Patients can be seen if they are ≥ 16 years old with known rheumatic disease or suspicion for rheumatic disease. All patients receive education and monitoring of transition readiness. We provide transition readiness education in 5 discrete modules (Fig 1); education materials are adapted from Got Transition Tm (Fig 2). All patients complete patient reported outcome measures (PRO’s). We maximize continuity of care in several ways: our adult rheumatologist meets pediatric patients who anticipate transfer to the transition clinic, she manages all transition clinic visits, and if possible, she migrates care to our institution’s associated adult rheumatology clinic. Demographics, PRO’s, transition readiness measures, and clinical outcomes are collected in a prospective longitudinal registry. IRB approval was obtained for this study.
Results: In 7 months, 65 patients visited the transition clinic (Table 1). 70.8% were new patients. Of these, we diagnosed 34.8% with a new rheumatic disease (rheumatoid arthritis (RA), mixed connective tissue disease, antiphospholipid syndrome, Raynaud phenomenon, spondyloarthritis (SpA), enteropathic arthritis, gout, Ehlers-Danlos syndrome, and linear morphea). 29.2% were transfers for known rheumatic disease of childhood onset (juvenile idiopathic arthritis (JIA), systemic lupus erythematosus, SpA, and Sjogren’s syndrome). Nine (13.8%) have scheduled upcoming visits with the adult rheumatologist in our affiliated adult rheumatology clinic. Four (6.2%) have completed durable transfer to our adult rheumatology clinic (defined as one or more scheduled and completed appointments). One (1.5%) patient has successfully transitioned to an outside adult rheumatologist.
Conclusion: We have successfully initiated an evidence-based transition clinic in a pediatric rheumatology academic institution that integrates the care of an adult rheumatologist. The transition clinic has diagnosed 16 new rheumatologic diagnoses in adolescence, eliminating the future need for transition to an adult provider. We have established 19 patients with our adult rheumatologist in the transition clinic, alongside our pediatric rheumatology clinic. We have transferred 9 patients to an adult rheumatology clinic, 8 to our associated adult rheumatology clinic, and 4 have completed a durable transition to date. Future research of this registry will analyze this cohort and the impact of this intervention on clinical outcomes and PRO’s.
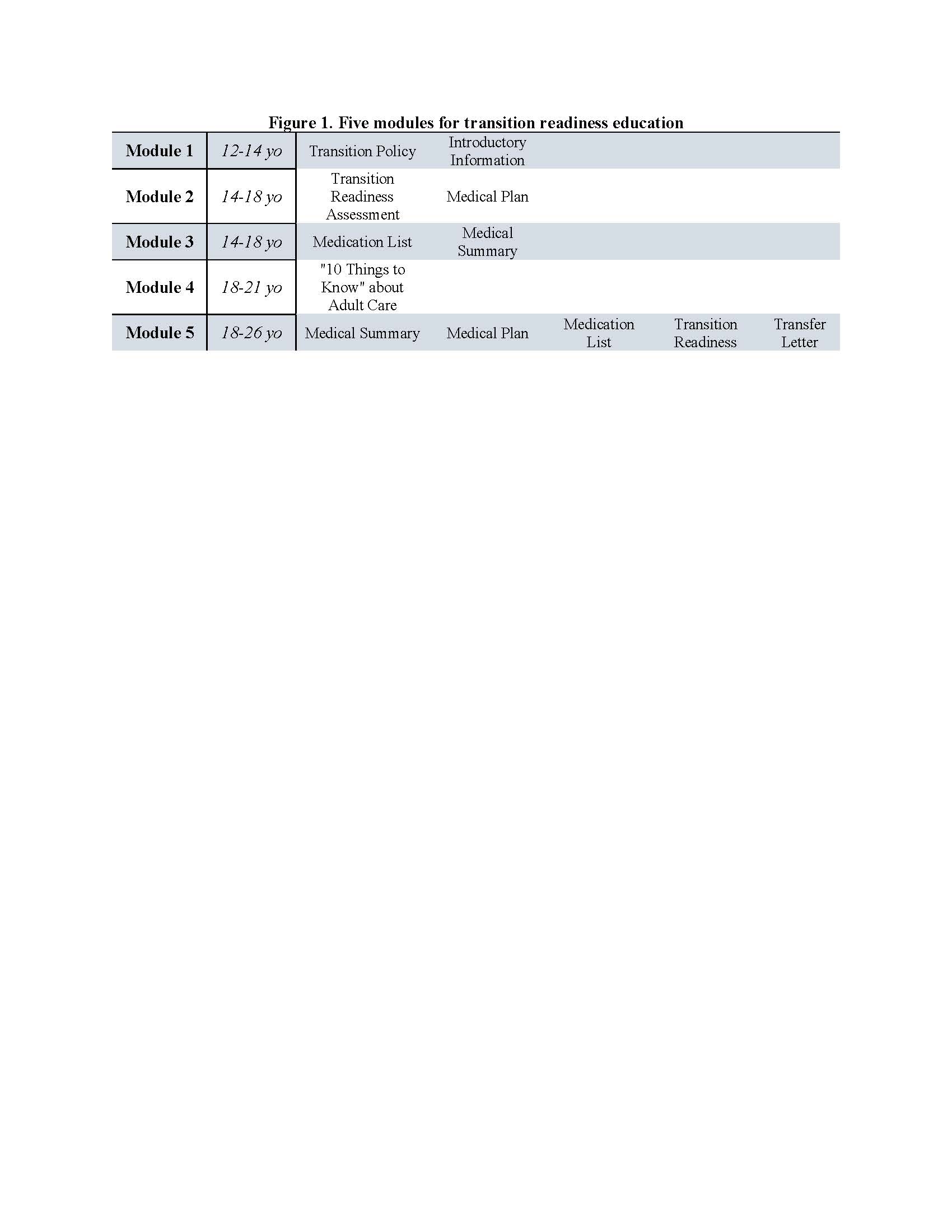
Figure 1
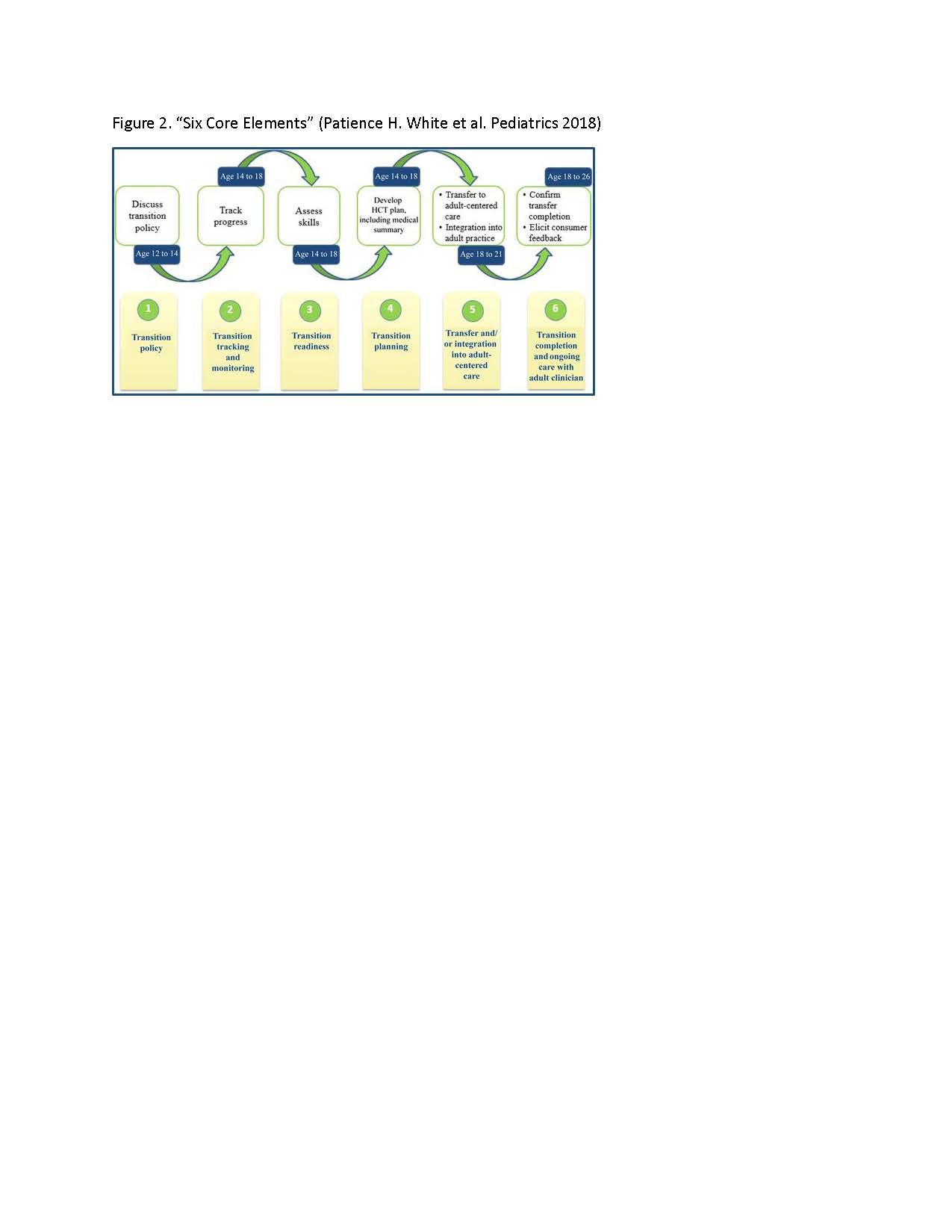
Figure 2
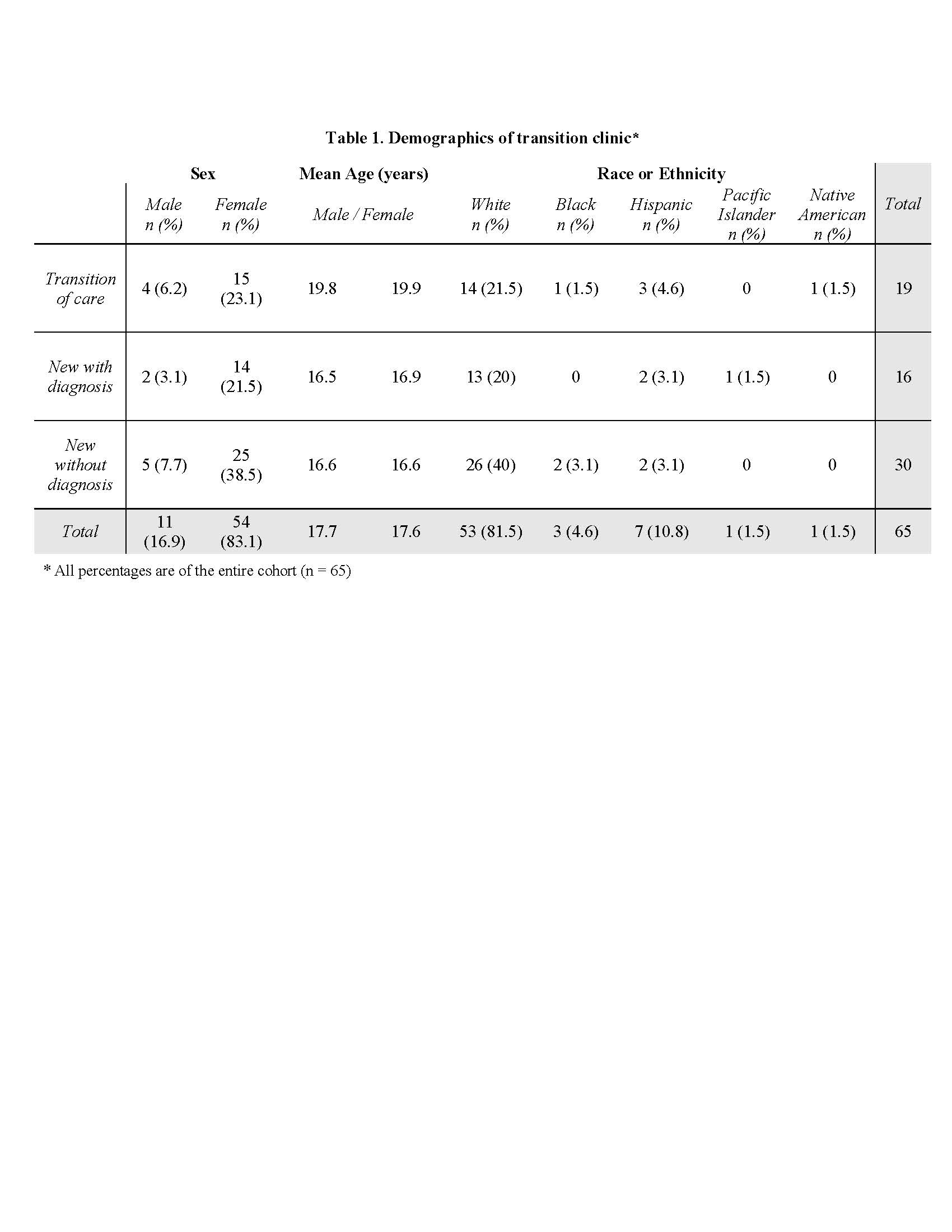
Table 1
To cite this abstract in AMA style:
Overbury R, Bohnsack J, Inman C, Stern S, James K, Clegg D, Frech T, Hersh A. Implementation of an Evidence-based Transition Clinic in a Pediatric Rheumatology Academic Institution [abstract]. Arthritis Rheumatol. 2019; 71 (suppl 10). https://acrabstracts.org/abstract/implementation-of-an-evidence-based-transition-clinic-in-a-pediatric-rheumatology-academic-institution/. Accessed .« Back to 2019 ACR/ARP Annual Meeting
ACR Meeting Abstracts - https://acrabstracts.org/abstract/implementation-of-an-evidence-based-transition-clinic-in-a-pediatric-rheumatology-academic-institution/