Session Information
Session Type: Abstract Submissions (ACR)
Background/Purpose: Current guidelines recommend treatment for rheumatoid arthritis (RA) be informed by a measure of disease activity such as the Disease Activity Score-28 (DAS28-CRP), which includes physician assessments of tenderness and swelling in joints. We explored the impact of basing disease activity measurement and treatment recommendations for RA patients on patient joint assessments rather than physician assessments.
Methods: 364 RA subjects enrolled in the Rheumatoid Arthritis Comparative Effectiveness Research (RACER) registry and their physicians performed independent and blinded exams of 28 joints for tenderness and swelling during routine clinic visits. Subjects assessed their own joints assisted by a web-based tool that provided illustrations and instructions. We measured discrepancies in the DAS28-CRP, disease activity categories and treatment recommendations (following American College of Rheumatology (ACR) guidelines for therapy adjustment) when based on patient vs. physician assessments. Treatment recommendations were compared with actual treatment decisions for 342 subjects.
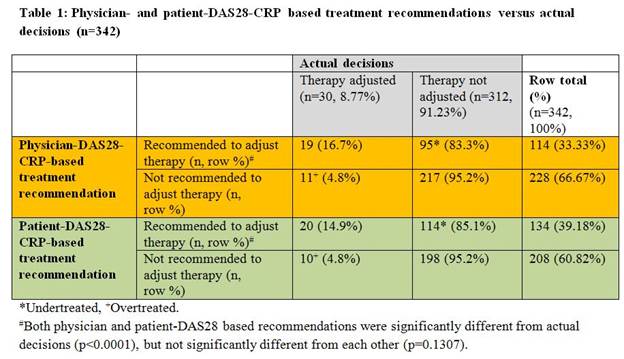
Results: Mean DAS28-CRP scores based on patient assessments were higher than when based on physician assessments (mean ±SD, 3.49 ±1.50 vs. 3.02 ±1.25; p<0.0001). In 56% of 364 cases, the patient and physician-based DAS28-CRP led to categorization in the same disease severity level; in 44% of cases the patient and physician-based scores led to discrepant categorizations. In 84% of cases the physician and patient-based scores would yield the same recommendation regarding therapy adjustment, but in 16% of cases they would yield different recommendations. When evaluating actual decisions against treatment recommendations based on ACR guidelines (n=342), only 8.77% of patients actually adjusted therapy, compared to 33.33% and 39.18% recommended to adjust therapy according to physician and patient DAS28-CRP, respectively (Table 1). Actual rates of therapy adjustment were low among those subjects recommended to adjust therapy (16.7% when assessed by physician DAS28-CRP and 14.9% when assessed by patient DAS28-CRP (Table 1)).
Conclusion: Although discrepancies in disease severity categorization occurred frequently (44% of the time), discrepancies in RA treatment recommendations arose less frequently (16% of the time) as a result of differences in patient and physician joint exams. Regardless of whether treatment recommendations were based on patient or physician joint exams, actual treatment decisions often appeared to be inconsistent with disease severity, primarily because therapy was often not adjusted despite > 3 months of moderate to high disease activity. Further research will explore disease and health-related outcomes associated with miscategorizing disease severity and under-treating RA patients.
Disclosure:
Y. Shaw,
Genentech and Biogen IDEC Inc.,
2;
D. Bang,
None;
H. Eng,
Genentech and Biogen IDEC Inc.,
2;
S. R. Wisniewski,
Genentech and Biogen IDEC Inc.,
2;
M. S. Roberts,
None;
M. C. Levesque,
Genentech and Biogen IDEC Inc.,
2,
UCB,
5,
AbbVie,
9,
Crescendo,
5,
Baxter Healthcare,
5.
« Back to 2013 ACR/ARHP Annual Meeting
ACR Meeting Abstracts - https://acrabstracts.org/abstract/impact-of-basing-rheumatoid-arthritis-disease-activity-measurement-and-treatment-recommendations-on-patient-instead-of-physician-joint-assessments/