Session Information
Date: Sunday, October 21, 2018
Session Type: ACR Poster Session A
Session Time: 9:00AM-11:00AM
Background/Purpose: Remission (REM) or minimal/low disease activity (LDA) is the treatment goal in Psoriatic Arthritis (PsA). There is no consensus on definitions of REM/LDA. Recently, composite measures of disease activity have been compared but this comparison did not address the patient’s perspective (ref).
The objectives were to assess frequency of REM/LDA using different definitions, and agreement between these definitions according to the patient’s and physician’s perspectives.
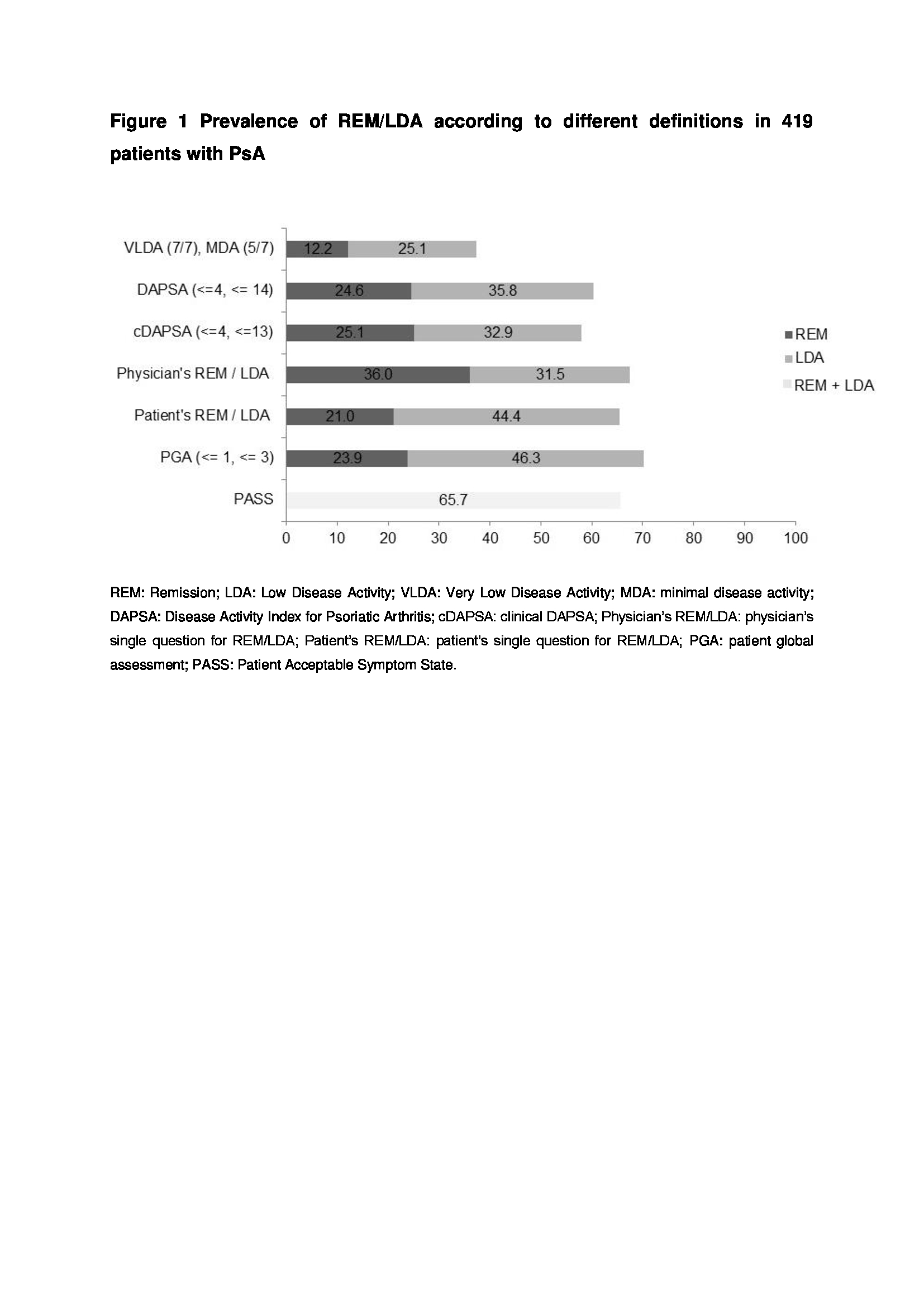
Methods: ReFlap (NCT03119805) is a cross-sectional study in 14 countries of consecutive adults with definite PsA and more than 2 years of disease duration. REM and LDA were defined using Very Low Disease Activity (VLDA), Minimal Disease Activity (MDA), Disease Activity in PSoriatic Arthritis (DAPSA), clinical DAPSA (cDAPSA) and Patient Global Assessment (PGA). Furthermore, REM and LDA were assessed using specific single questions for the physician and the patient (Figure 1: physician and patient REM/LDA).
Proportions achieving each REM/LDA criterion were calculated. The agreement between the tested definitions was assessed by Venn diagram and calculation of kappa and prevalence-adjusted and bias-adjusted kappa (PABAK).
Results: Of 466 patients, 419 had data available for all definitions of REM/LDA: 212 (51.3%) were male, mean age was 53.9±12.6 years and mean disease duration 11.3±8.4 years, 59.0% were taking a biologic. Disease activity was moderate: 9.5% had a Body Surface area of psoriasis≥5%, mean Tender and Swollen Joint Counts were respectively 4.9±9.7 and 2.3±7.2. The frequency of REM varied from 12.2% (VLDA) to 21.0% (Physician REM question) and of LDA from 25.1% (MDA) to 46.3% (PGA≤3) (Figure 1). Agreement was moderate between the composite scores for REM (kappa DAPSA/VLDA 0.57, cDAPSA/VLDA 0.59). Agreements were lower for LDA whatever the definition used. Agreement between patient-defined REM/LDA and composite scores was only moderate. In particular, 36/88 (40.9%) of patients in patient-perceived REM were not in REM according to any composite score. Moreover, agreement between patient and physician REM occurred in 58/148 (39.0%) patients (Figure 2).
Conclusion: In this unselected population, REM/LDA was frequently attained. VLDA/MDA was a more stringent definition than DAPSA-based REM/LDA. Patient-assessed REM/LDA was similar in terms of prevalence to DAPSA, though agreement between patients and composite scores was only moderate. Further studies of patients’ expectations are needed.
Reference. van Mens LJJ et al.Ann Rheum Dis. 2018

To cite this abstract in AMA style:
Gorlier C, Puyraimond-Zemmour D, Coates LC, Orbai AM, Kiltz U, Leung YY, Palominos P, Cañete JD, Scrivo R, Balanescu AR, Dernis E, Tälli S, Ruyssen-Witrand A, Soubrier M, Aydın SZ, Eder L, Gaydukova I, Lubrano E, Richette P, Husni ME, de Wit M, Smolen JS, Gossec L. How to Define Remission and Low Disease Activity in Psoriatic Arthritis? an Analysis of 419 Patients with a Double Perspective, Based on Composite Scores and Patients’ and Physicians’ Perspectives [abstract]. Arthritis Rheumatol. 2018; 70 (suppl 9). https://acrabstracts.org/abstract/how-to-define-remission-and-low-disease-activity-in-psoriatic-arthritis-an-analysis-of-419-patients-with-a-double-perspective-based-on-composite-scores-and-patients-and-physicians-perspecti/. Accessed .« Back to 2018 ACR/ARHP Annual Meeting
ACR Meeting Abstracts - https://acrabstracts.org/abstract/how-to-define-remission-and-low-disease-activity-in-psoriatic-arthritis-an-analysis-of-419-patients-with-a-double-perspective-based-on-composite-scores-and-patients-and-physicians-perspecti/