Session Information
Session Type: Poster Session C
Session Time: 9:00AM-11:00AM
Background/Purpose: Immunothrombosis is a critical pathological feature of fulminant COVID-19 pneumonia in which immunosuppression with common immunomodulatory agents such as corticosteroids, IL-6 receptor blockers, and JAK inhibitors have shown benefit [1–4].The basis for the efficacy of immunomodulation in the face of potentially critical viral pneumonia remains poorly understood. This study ascertained the impact of age and obesity, both of which increase thrombotic tendencies, on survival following baricitinib therapy for severe COVID-19 in the Phase III COV-BARRIER 3 trial where baricitinib improved survival compared to placebo [4].
Methods: We performed a post-hoc analysis of the COV-BARRIER multicentre double-blind randomized study of baricitinib versus placebo with an assessment of 28-day mortality (a key secondary outcome in the trial) in 1525 hospitalized COVID-19 adult patients. Age was categorized into < 65 years and ≥65 years, and BMI was categorized d into < 25 kg/m2 (normal), and ≥ 25 kg/m2 (high). To assess the incidence rate ratios of mortality in the different subgroups, we employed the assumption of a Poisson distribution. All-cause mortality by day 28 was evaluated in a cox-regression analysis (adjusted to age) in three different groups according to BMI (< 25 kg/m2, 25-30 kg/m2, and > 30 kg/m2).
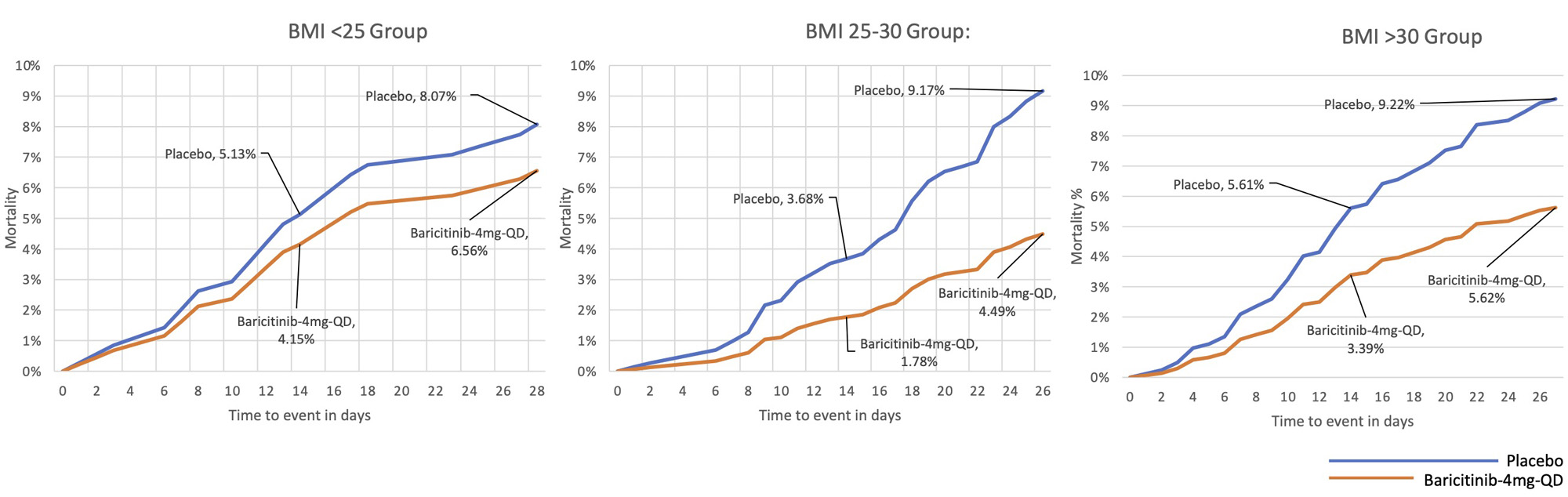
Results: As reported in COV-BARRIER 3 data [4], all-cause mortality by day 28, a key-secondary endpoint, was 8% (n=62) in the baricitinib arm and 13% (n=100) for placebo (PBO), HR 0.57 [95% CI 0.41-0.78].However, we found that in the normal BMI group, irrespective of age, baricitinib therapy did not show a significant survival advantage when compared to PBO [IRR of 1.89 (95% CI: 0.49 to 7.28) and 0.95 (95% CI: 0.46 to 1.99) for < 65yo and ≥ 65yo respectively]. In patients with high BMI, mortality in the baricitinib group was 5.3% (22/418) in < 65 years old (yo) and 20.0% (40/200) in ≥ 65yo. For PBO, mortality rates were 9.9% (43/435) in < 65yo and 30.5% (53/174) in ≥ 65yo. The Incidence rate ratio (IRR) was 0.53 (95% CI: 0.32 to 0.87) and 0.66 (95% CI: 0.46 to 0.94) for the respective age categories. The 28-all-cause-mortality for BMI over 30 was 9.22% for baricitinib and 5.62% for PBO [HR= 0.6, (5.6%vs 9.2%), p< 0.05], while for BMI < 25, the difference between 28-all-cause-mortality between baricitinib and PBO arms was not significant [(6.6% vs 8.1), p>0.05] (Figure 1).
Conclusion: Baricitinib was associated with significantly lower mortality in patients with high BMI and older subjects. Both BMI and age are associated with immunothrombosis, and the protective effect of JAK inhibition in such groups is remarkable given the reports of thrombosis with JAK inhibition in rheumatoid arthritis.
References:
1- Nicolai L, Leunig A, Brambs S, et al.Journal of Thrombosis and Haemostasis 2021;19:574–81.
2- Ranucci M, Ballotta A, di Dedda U, et al. Journal of Thrombosis and Haemostasis 2020;18:1747–51.
3- Kalil AC, Patterson TF, Mehta AK, et al.New England Journal of Medicine 2021;384:795–807.
4- Marconi VC, Ramanan A V., de Bono S, et al.Lancet Respir Med 2021;9:1407–18.
To cite this abstract in AMA style:
David P, Ben-Shabbat N, Hen O, Amital H, watad A, McGonagle D. Higher Body Mass Index and Older Age, Both of Which Are Linked to Immunothrombosis Are Associated with Improved Survival with Baricitinib Therapy in COVID-19 Pneumonia [abstract]. Arthritis Rheumatol. 2023; 75 (suppl 9). https://acrabstracts.org/abstract/higher-body-mass-index-and-older-age-both-of-which-are-linked-to-immunothrombosis-are-associated-with-improved-survival-with-baricitinib-therapy-in-covid-19-pneumonia/. Accessed .« Back to ACR Convergence 2023
ACR Meeting Abstracts - https://acrabstracts.org/abstract/higher-body-mass-index-and-older-age-both-of-which-are-linked-to-immunothrombosis-are-associated-with-improved-survival-with-baricitinib-therapy-in-covid-19-pneumonia/