Session Information
Session Type: ACR Abstract Session
Session Time: 11:00AM-12:30PM
Background/Purpose: Giant cell arteritis (GCA) is the most common form of vasculitis of large arteries affecting people older than 50 years. Temporal artery biopsy (TAB) is still considered as the gold standard for GCA diagnosis but it is invasive and its sensitivity ranges from 39 to 86%.Color Doppler Ultrasonography and PET-scanner have been proposed as alternative methods for GCA diagnosis but are not widespread in routine clinical practice. Recent recommendations suggest the use of MRI as an alternative method for GCA diagnosis. To our knowledge, there is no evaluation of 3D sequences in the diagnosis of GCA
Methods: We decided to evaluate the diagnostic performance of pre and post-contrast fat-suppressed 3D-Fast Spin echo T1-weighted black-blood magnetic resonance imaging (CUBE-T1), of the external carotid in the diagnosis process of GCA.
Results: Thirty-two patients (7 men, 25 women, mean±SD age 70.2±12.1 years) were included. The final diagnosis, blinded to CUBE T1 results, was GCA for 10 of them. 3D CUBE T1 displayed the arteries wall clearly, allowing an easy identification of parietal enhancement and the 3D TOF coregistration was helpful in image analysis. Intra- and inter-observer agreement for mural enhancement on CUBE T1 was 1 and 0.84, respectively.
Height of the 10 patients with GCA had a strong mural enhancement in CUBE-T1 (Figure 1), while none of the 22 patients without GCA had mural enhancement in MR images. Therefore, sensitivity was 80% and specificity was 100 %. The positive predictive value of post-contrast CUBE T1 was 100% and the negative predictive value was 92%. In our cohort, only 6 of the 10 GCA patients had a positive TAB. Therefore sensitivity of TAB was 60%. If TAB was used as the reference standard, MRI yielded a sensitivity of 100%. Two patients with a final diagnosis of GCA despite normal TAB had an arteritis on MRI and vessel enhancement was observed in occipital artery only for one patient.
Conclusion: We here demonstrate the feasibility and accuracy of a 3D post-contrast CUBE-T1 in the diagnosis of GCA. Indeed, we observed a sensitivity of 80%, which is higher than the 64.1% that was observed by Rhéaume et al. with 2D sequences on his series of 172 patients. We hypothesize that 3D MRI acquisition allowing multiplanar reconstructions together with the 3D TOF coregistration might explain the higher sensitivity and the excellent reproducibility. The reproducibility and short scan duration is a clear advantage of CUBE-T1 sequences with sub-millimetric voxels acquisition. Additional studies are required to confirm our preliminary results.
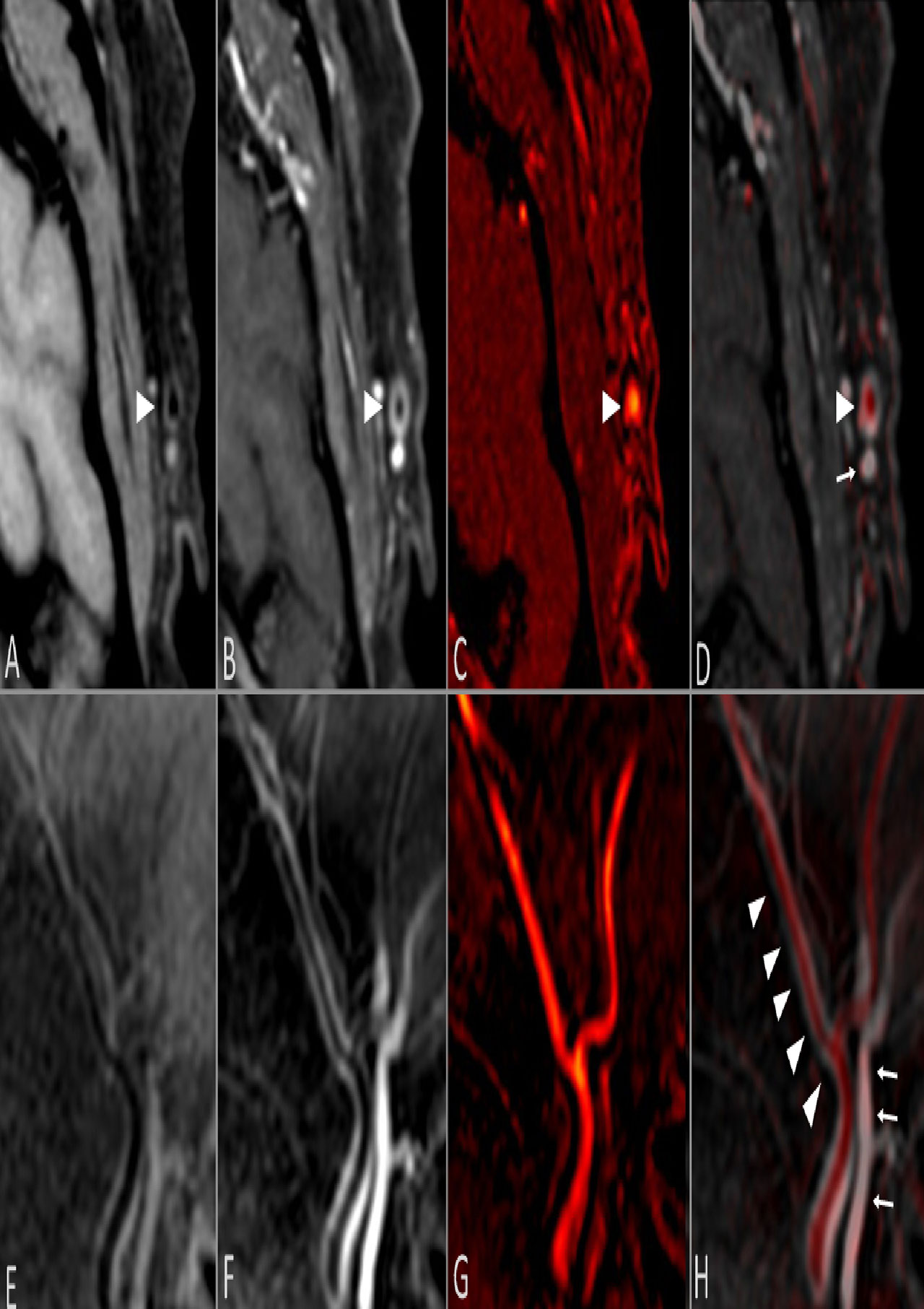
Figure 1
Axial and sagittal reconstructions of CUBE T1 sequence before -A and E respectively- and after contrast injection -B and F respectively-. 3D TOF sequence in axial and sagittal plane -C and G respectively- coregistered with post-contrast CUBE T1 sequence -D and H respectively-, allowing a differentiation between the temporal artery in red -arrowhead- -C, G- and the temporal vein -arrows- -D, H-. Strong mural enhancement of the temporal artery -arrowhead- -B, D, F, H-.
To cite this abstract in AMA style:
rodriguez C, Ben Hassen W, Seners P, Oppenheim C, Régent A. High Resolution 3D Fast Spin-Echo T1 Black-Blood Imaging for the Diagnosis of Giant Cell Arteritis [abstract]. Arthritis Rheumatol. 2019; 71 (suppl 10). https://acrabstracts.org/abstract/high-resolution-3d-fast-spin-echo-t1-black-blood-imaging-for-the-diagnosis-of-giant-cell-arteritis/. Accessed .« Back to 2019 ACR/ARP Annual Meeting
ACR Meeting Abstracts - https://acrabstracts.org/abstract/high-resolution-3d-fast-spin-echo-t1-black-blood-imaging-for-the-diagnosis-of-giant-cell-arteritis/