Session Information
Date: Saturday, November 12, 2022
Title: Health Services Research Poster I: Lupus, RA, Spondyloarthritis and More
Session Type: Poster Session A
Session Time: 1:00PM-3:00PM
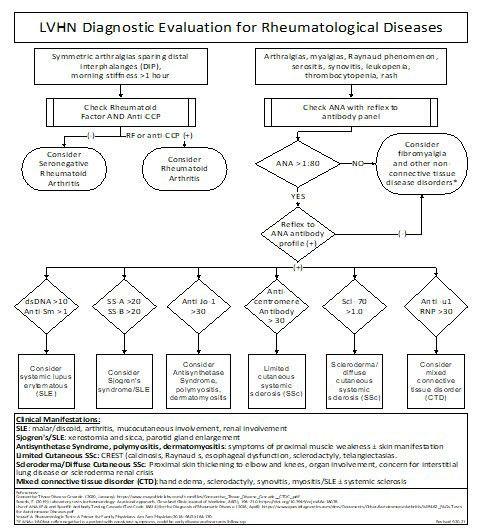
Background/Purpose: In 2005 Lehigh Valley Health Network (LVHN) instituted order sets for ANA serologic reflex testing with the objective to facilitate more efficient patient work-up of a positive ANA. Since then, LVHN continues to offer 3 ANA labs panels including: ANA Alone, ANA with Reflex with ANA > 1:80 reflexed by adding serologic testing, and Comprehensive ANA which includes ANA and at the same time serologic testing. This serologic testing panel includes Sjogren’s antibodies, dsDNA, RNP, Smith, and SCL 70. Benefits of the ANA with Reflex panel include a single visit to the laboratory, and a more rapid cost-effective diagnostic assessment.
The goal of this quality improvement project was to determine ANA panel order frequency and appraisal of educational and EMR interventions for more efficient and cost-effective testing.
Methods: Review of inpatient EMR records found a high frequency of Comprehensive ANA test results with a negative ANA. An education pathway was created that delineated an approach of tests to order starting with ANA with Reflex when suspecting a rheumatological disorder (Fig 1). This was directed towards departments inappropriately ordering more Comprehensive ANA’s: neurology, orthopedics, family medicine and internal medicine. Subsequent data review demonstrated no change in the percentage each of the ANA panel orders. This led to LVHN Test Utilization Committee’s approval for removal of the Comprehensive ANA order from the inpatient EMR for all specialties except rheumatology. The frequency of orders of the ANA with Reflex and Comprehensive ANA were compared for three months before and three the months after this EMR intervention.
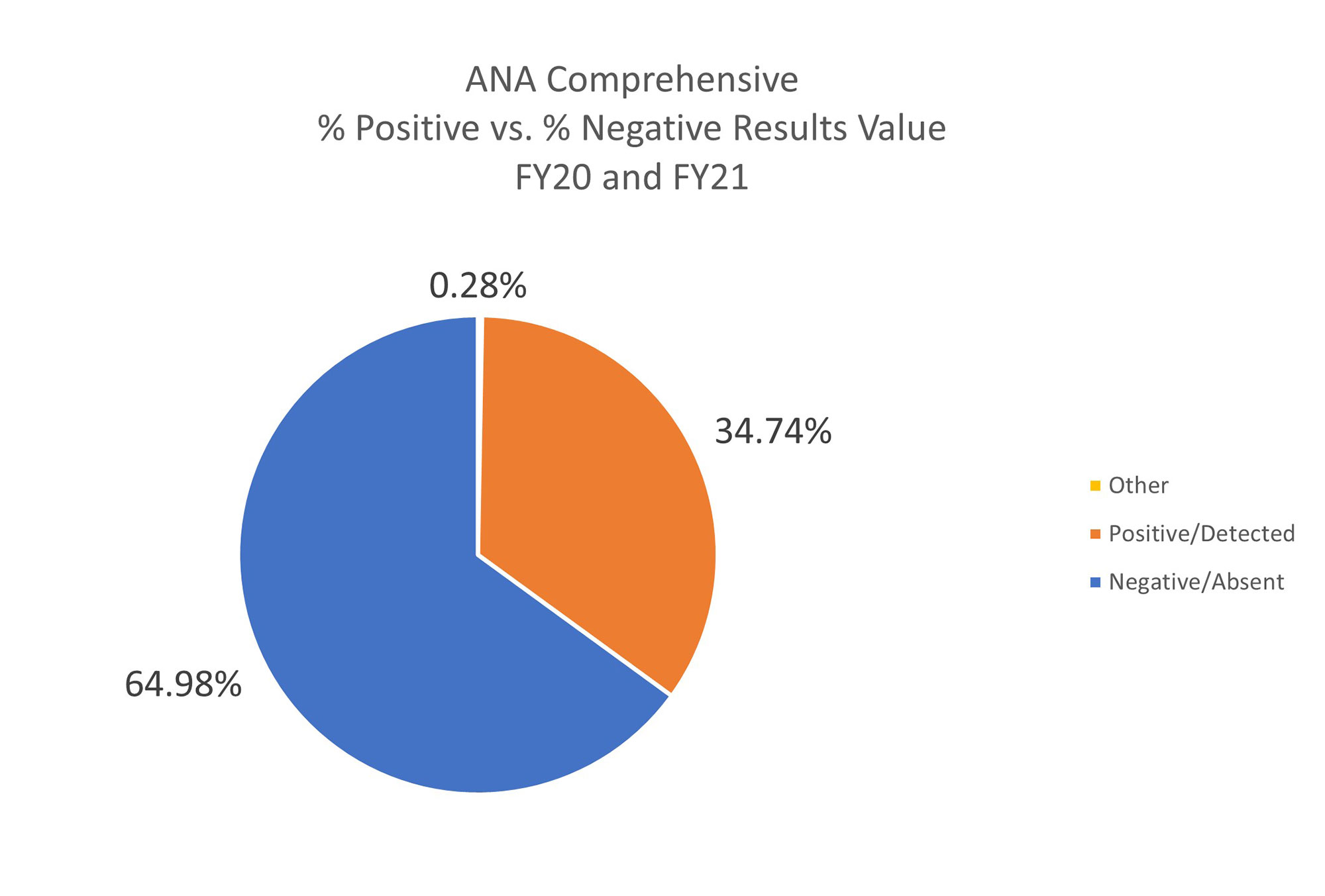
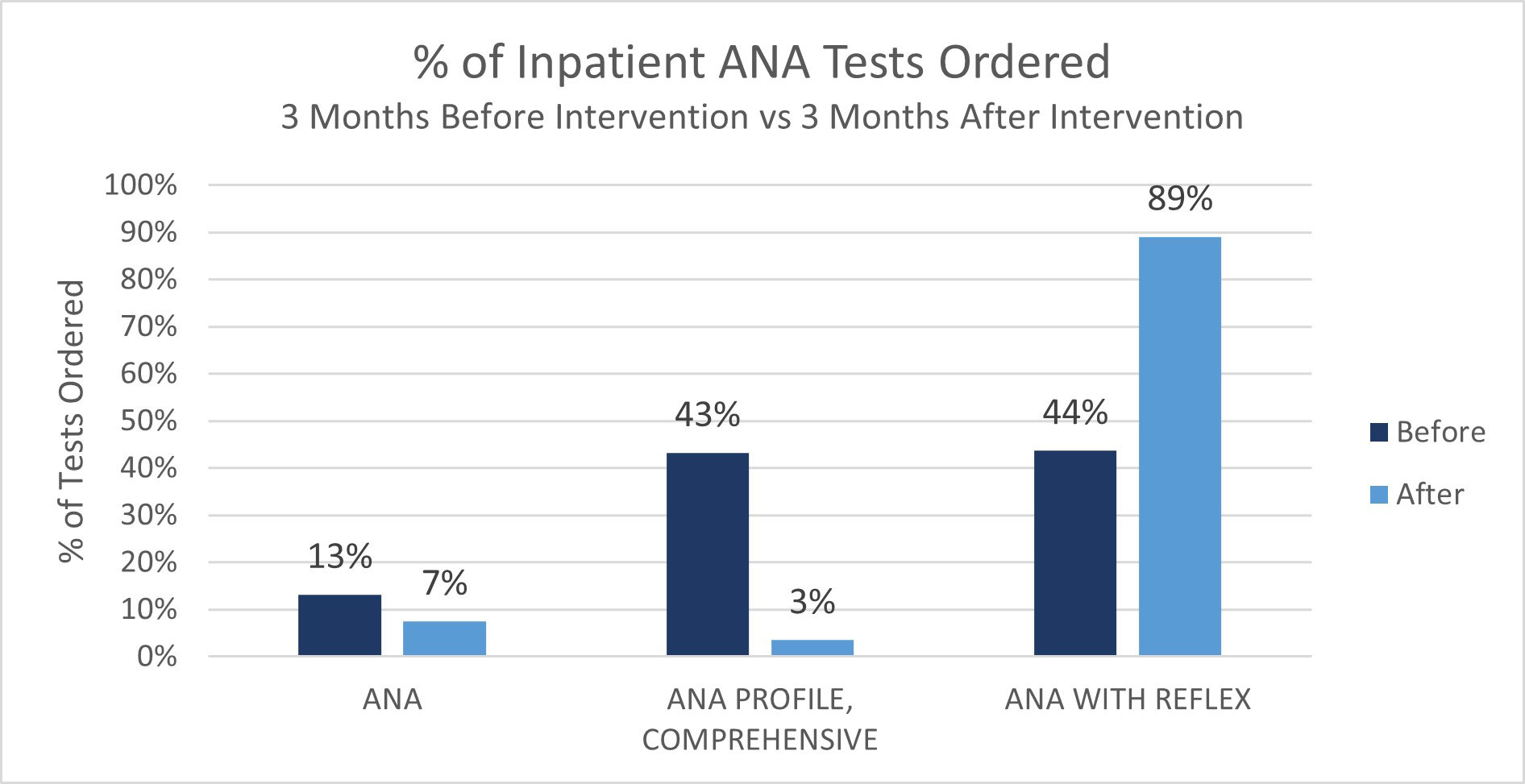
Results: This was LVHN’s first appraisal of ANA panel order frequency. The Comprehensive ANA serology was overutilized with 64.98% of Comprehensive ANA ordered being ANA negative, and in these cases the serology panel was unnecessary (Fig 2). The EMR intervention of removing the inpatient Comprehensive ANA resulted in a decrease in the Comprehensive ANA testing with an associated increase in ANA with Reflex. The number of Comprehensive ANA decreased from 181 to 14 and the number of ANA with Reflex increased from 183 to 358. The ANA with reflex became the predominant ANA test ordered at 89% (Fig 3). A small number of Comprehensive ANA panels were ordered by rheumatology. We estimated this inpatient intervention saved the healthcare system $26,000 over 3 months. EMR removal of ANA alone panel has not been implemented yet. The ANA Alone results were approximately 60% normal ANA’s and 40% abnormal.
Conclusion: This quality improvement project detected rheumatic test overutilization and improvement with the removal of the EMR Comprehensive ANA serology panel combined with provider education. LVHN’s approach to ANA testing can be replicated in healthcare systems across the country to reduce cost burden as well as improve efficiency. Our future ANA panel assessments and EMR interventions will focus on improving ANA Alone panels and outpatient ANA testing.
References Tonutti, E., Bizzaro, N., Morozzi, G. et al. The ANA-reflex test as a model for improving clinical appropriateness in autoimmune diagnostics. Autoimmun Highlights 7, 9 (2016).
To cite this abstract in AMA style:
Goyal S, kanakrieh Y, O'Brien M, Slenker A, Zaffiri K, Ross J. Health System Improvement in Inpatient ANA and Serologic Test Utilization [abstract]. Arthritis Rheumatol. 2022; 74 (suppl 9). https://acrabstracts.org/abstract/health-system-improvement-in-inpatient-ana-and-serologic-test-utilization/. Accessed .« Back to ACR Convergence 2022
ACR Meeting Abstracts - https://acrabstracts.org/abstract/health-system-improvement-in-inpatient-ana-and-serologic-test-utilization/