Session Information
Date: Tuesday, November 15, 2016
Title: Spondylarthropathies and Psoriatic Arthritis – Clinical Aspects and Treatment - Poster III
Session Type: ACR Poster Session C
Session Time: 9:00AM-11:00AM
Background/Purpose: Patients with psoriatic arthritis (PsA) are associated with higher cardiovascular (CV) risks. The efficacy of established CV risk scores for predicting CV risks in PsA patients is unknown. The aim of this study is to evaluate the efficacy of different CV risk scores and their European League Against Rheumatism (EULAR) modified versions for discriminating the presence of coronary atherosclerosis evaluated by coronary Computed Tomography Angiography (CTA) in PsA patients.
Methods: Four different CV risk scores namely Framingham risk score (FRS), American College of Cardiology and American Heart Association (ACC/AHA) 10-year atherosclerotic cardiovascular disease (ASCVD), QRISK II and SCORE, together with their EULAR recommended modified versions (1.5 multiplication) were calculated. Presence of overall plaque (P+) and mixed plaque/non-calcified plaque (MP/NCP+), were identified by CTA.
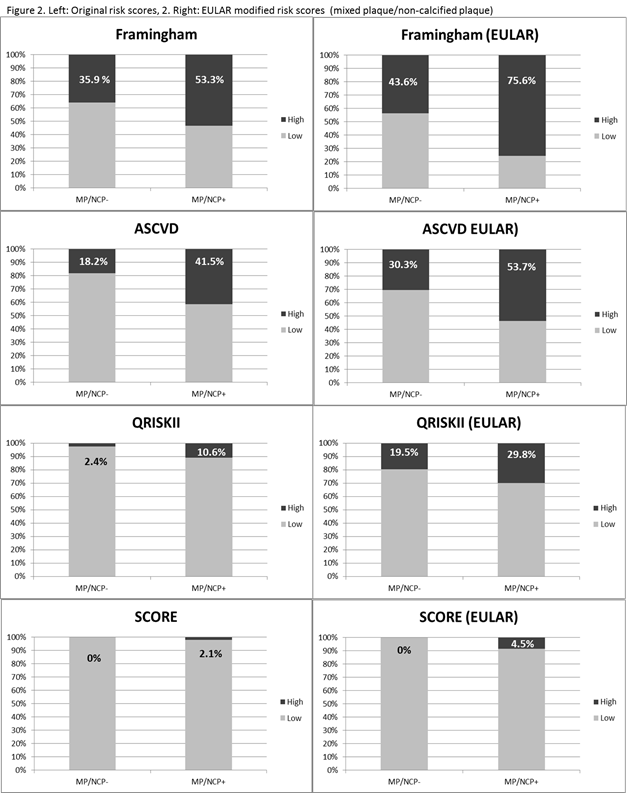
Results: 88 PsA patients [50 ¡Ó 11, male: 54(61.4%)] underwent CTA were recruited. 84, 74, 88 and 88 patients were eligible to calculate FRS, ASCVD, QRISKII and SCORE respectively. All CV risk scores were significantly higher in both P+ and MP/NCP+ patients [FRS: P+ (13.5 ¡Ó 8.7 vs 6.5 ¡Ó 5.3; p<0.001), MP/NCP+ (13.7 ¡Ó 9.0 vs 7.4 ¡Ó 5.7; p<0.001); ASCVD: P+ (7.0 ¡Ó 5.3 vs 3.4 ¡Ó 3.4; p<0.001), MP/NCP+ (7.1 ¡Ó 5.5 vs 3.9 ¡Ó 3.6; p=0.005); QRISKII: P+ (9.6 ¡Ó 7.8 vs 6.4 ¡Ó 6.6; p=0.047), MP/NCP+ (9.9 ¡Ó 8.2 vs 6.5 ¡Ó 6.3; p=0.035); SCORE: P+ (1.4 ¡Ó 1.4 vs 0.5 ¡Ó 0.8; p=0.001), MP/NCP+ (1.4 ¡Ó 1.4 vs 0.6 ¡Ó 1.0; p=0.004)]. Areas under the receiver operating characteristic (ROC) curves, differentiating P+ and MP/NCP+, were 0.77 (0.67 ¡V 0.88 p<0.001) and 0.73 (0.62 ¡V 0.84 p<0.001) for FRS, 0.76 (0.636 ¡V 0.87 p<0.001) and 0.72 (0.60 ¡V 0.84 p=0.001) for ASCVD, 0.65 (0.53 ¡V 0.78, p=0.018) and 0.64 (0.52 ¡V 0.76 p=0.026) for QRISKII, 0.72 (0.614 ¡V 0.831 p<0.001) and 0.68 (0.56 ¡V 0.79 p=0.005) for SCORE, respectively. 38(45.2%), 23(31.1%), 6(6.8%) and 1(1.1%) patients were classified as having high CV risks according to FRS>10%, ASCVD>7.5%, QRISK II>20% and SCORE>5% respectively. By applying the EULAR multiplication factor, 51(60.7%), 32(43.2%), 22(25%) and 4(4.5%) patients were reclassified as having high CV risks. The sensitivity of FRS>10% increased from 56.9% to 76.5% for P+ (Figure 1), and from 53.3% to 75.6% for MP/NCP+ (Figure 2). Other risk scores generally underestimated coronary atherosclerosis (Figure 1&2).
Conclusion: FRS was better correlated with coronary atherosclerosis than other CV risk scores. EULAR modification further improved the sensitivity of FRS.

To cite this abstract in AMA style:
LAM HM, Shen J, SHANG Q, CHENG TH, LI E, WONG KT, TAM LS. Framingham Risk Score Discriminates Coronary Atherosclerosis in Psoriatic Arthritis Patient Better Than Other Cardiovascular Scores Do [abstract]. Arthritis Rheumatol. 2016; 68 (suppl 10). https://acrabstracts.org/abstract/framingham-risk-score-discriminates-coronary-atherosclerosis-in-psoriatic-arthritis-patient-better-than-other-cardiovascular-scores-do/. Accessed .« Back to 2016 ACR/ARHP Annual Meeting
ACR Meeting Abstracts - https://acrabstracts.org/abstract/framingham-risk-score-discriminates-coronary-atherosclerosis-in-psoriatic-arthritis-patient-better-than-other-cardiovascular-scores-do/