Session Information
Date: Tuesday, November 12, 2019
Title: Osteoporosis & Metabolic Bone Disease – Basic & Clinical Science Poster
Session Type: Poster Session (Tuesday)
Session Time: 9:00AM-11:00AM
Background/Purpose: Osteoporosis-related fragility fractures contribute to significant morbidity and mortality. The risk of subsequent hip fracture is significantly increased after initial fracture, with some reports suggesting rates of recurrent fractures in hip and spine to be 41% and 45% at 1-year, respectively1. Hip fractures plateaued between 2002-2012, yet increased between 2013-2015 resulting in an estimated 11,000 additional fractures2. Despite widely available access to Dual-energy X-ray absorptiometry (DEXA) and treatment, this effect may be due to low rates of screening and treatment3. The purpose of this study was to identify the most common initial and secondary fractures, associated mortality, and frequency of screening and treatment.
Methods: Adults aged 65 and older diagnosed with fragility fracture at Lutheran General Hospital from January 2012 to January 2017 were included in this analysis. Fragility fractures, defined as wrist, humerus, vertebral, hip, and pelvis, were identified with ICD9/ICD10 codes, along with demographic and clinical characteristics from the Advocate Health Care EMR system. Univariate analysis for continuous and categorical variables were conducted. Logistic regression was applied to examine the association of demographic characteristics and risk of fragility fractures. A two-tailed P level of .05 was considered statistically significant in all analyses. All analyses were performed using SAS 9.4.
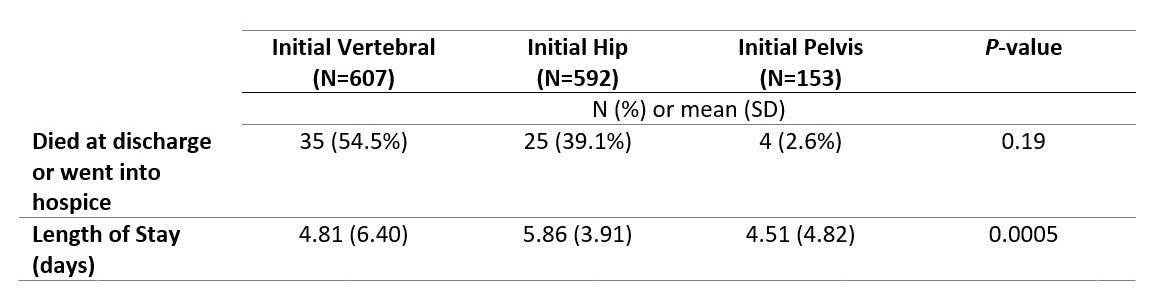
Results: A total of 1,424 initial and 137 secondary fragility fractures were identified. For initial fractures, vertebral was most common (607, 42.63%), closely followed by hip (592, 41.92%), and pelvis (153, 12.08%). The majority of initial fracture patients were females (1021, 71.7%), Caucasians (1209, 84.9%) and the mean age was 82.1-years-old (range: 66-105). DEXA and treatment with anti-resorptive medications were recorded at time of initial fracture among 17.6% and 1.9% of patients, respectively. DEXA and treatment for patients with recurrent fractures were recorded among 27% and 31% of patients, respectively. There were no statistically significant differences for in-hospital all-cause mortality among vertebral, hip, and pelvic fractures.
Conclusion: Vertebral, hip, and pelvic fractures are a common cause of initial fragility fracture in those over age 65. Pelvic fractures may represent an under-reported cause of initial fragility fracture with similar rates of morbidity compared to hip and vertebral fractures. Rates of screening and treatment are low after initial and recurrent fractures. Future studies aimed investigating barriers to primary and secondary fracture prevention and treatment are warranted.
References:
- Kanis JA, Johansson H, Oden A, Harvey NC, Gudnason V, Sanders KM, et al. Characteristics of recurrent fractures. Osteoporosis Int 2018; 29(8): 1747-1757.
- Lewiecki EM, Wright NC, Curtis JR, Siris E, Gagel RF, Saag KG, et al. Hip fracture trends in the United States, 2002 to 2015. Osteoporosis Int 2018; 29(3):717-722.
- Nguyen ET, Posas-Mendoza T, Siu AM, Ahn HJ, Choy SY, Lim Sy. Low rates of osteoporosis treatment after hospitalization for hip fracture in Hawaii. Osteoporosis Int 2018; 29(8):1827-1382.

To cite this abstract in AMA style:
Kneeland R, Wahle K, Gill I, Liu Y, Starosta M. Fragility Fractures in a Community Setting: Clinical Characteristics, Care Gaps, and Outcomes [abstract]. Arthritis Rheumatol. 2019; 71 (suppl 10). https://acrabstracts.org/abstract/fragility-fractures-in-a-community-setting-clinical-characteristics-care-gaps-and-outcomes/. Accessed .« Back to 2019 ACR/ARP Annual Meeting
ACR Meeting Abstracts - https://acrabstracts.org/abstract/fragility-fractures-in-a-community-setting-clinical-characteristics-care-gaps-and-outcomes/