Session Information
Date: Monday, November 8, 2021
Title: Osteoporosis & Metabolic Bone Disease – Basic & Clinical Science Poster (1135–1149)
Session Type: Poster Session C
Session Time: 8:30AM-10:30AM
Background/Purpose: Glucocorticoids are commonly prescribed for a multitude of indications, yet have many side effects, one of which is glucocorticoid induced osteoporosis (GIOP). The 2017 ACR GIOP guidelines were developed to help improve screening and management of osteoporosis for this specific population. In this study, we investigated if patients at a large rural academic center receiving glucocorticoids were appropriately monitored with DXA based on the 2017 ACR screening guidelines.
Methods: Through a retrospective electronic chart review we evaluated patients in a rural tertiary medical center in central Pennsylvania who met specific inclusion criteria: 40 years or older who received a prescription for 2.5mg of a prednisone equivalent ≥ 90 days starting January 1, 2018 – December 31, 2019. Patients that met criteria were reviewed for DXA orders between 2018 – 2020, the department that ordered the steroids, the DXA ordering department, and if a DXA had been completed. Logistic regression models were used to test for overall and pairwise associations between steroid ordering departments and whether DXAs were ordered and whether DXAs were completed.
Results: The total number of charts that met the initial electronic screening criteria was 6022. Of those, 1000 charts were randomly selected for manual review via a computer generated simple random sample. Of those 1000 patients, 673 met the inclusion criteria. Overall, 262 of 673 patients (38.9%) had DXAs ordered in the three-year period and 187 had DXAs completed (27.8%). If the most recent steroid order was from a rheumatology provider, 45.1% of patients had a DXA ordered and 34.0% had a DXA completed. Patients whose steroid was ordered by rheumatology had significantly more DXAs ordered than patients whose steroid orders came from all other departments combined (45.1% vs. 33.8%, p = 0.0028). In pair-wise comparisons against individual departments, patients from rheumatology had more DXA orders than hematology/oncology (45.1% vs 12.8%, p = 0.0005), and primary care (45.1% vs 35.1%, p = 0.0354). There were no statistically significant differences between rheumatology, gastroenterology, neurology, surgery, or pulmonary medicine. Patients whose steroid was ordered by rheumatology had significantly more DXAs completed than patients whose steroid orders came from all other departments combined (34.0% vs. 22.6%, p = 0.0011).
Conclusion: There was significant variability between different specialties in ordering of DXA scans. While the rheumatology department was more compliant with ACR guidelines when all other departments are combined, they still are screening fewer than 50% of patients who meet the ACR guidelines. This demonstrates a care gap in osteoporosis screening in this population. We plan to analyze the remaining 5022 patient charts to determine how many meet criteria for DXA screening and expound on our preliminary results. We also hypothesize that the observed trends in interdepartmental differences will lead to more robust conclusions when analysis is completed with the full population. Additionally, we intend to implement a medical chart notification that would alert providers to consider DXA screening in appropriate patients.
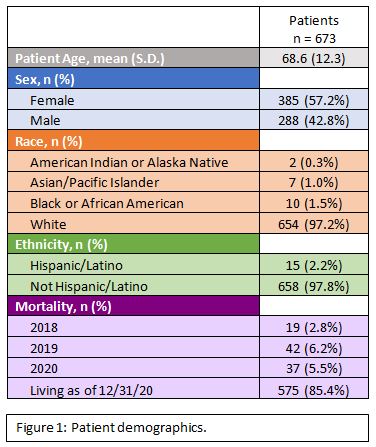 Patient demographics
Patient demographics
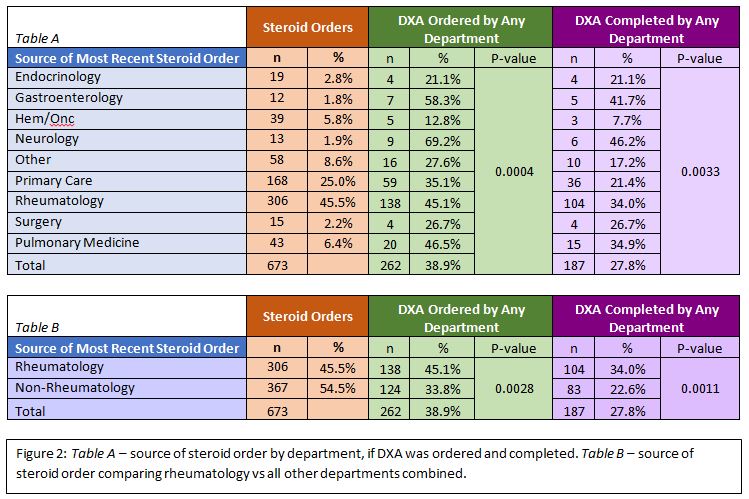 Figure 2: Table A – source of steroid order by department, if DXA was ordered and completed. Table B – source of steroid order comparing rheumatology vs all other departments combined.
Figure 2: Table A – source of steroid order by department, if DXA was ordered and completed. Table B – source of steroid order comparing rheumatology vs all other departments combined.
To cite this abstract in AMA style:
Chop A, Kupuraju R, Patel R, Salava K, Duggirala M, Baburaj A, Berger A, Brown J, Bulbin D. Fracture Risk in DXA-Appropriate Patients on Glucocorticoids: Is Everyone Tested According to Screening Guidelines? [abstract]. Arthritis Rheumatol. 2021; 73 (suppl 9). https://acrabstracts.org/abstract/fracture-risk-in-dxa-appropriate-patients-on-glucocorticoids-is-everyone-tested-according-to-screening-guidelines/. Accessed .« Back to ACR Convergence 2021
ACR Meeting Abstracts - https://acrabstracts.org/abstract/fracture-risk-in-dxa-appropriate-patients-on-glucocorticoids-is-everyone-tested-according-to-screening-guidelines/