Session Information
Session Type: ACR Poster Session C
Session Time: 9:00AM-11:00AM
Background/Purpose: A valid flare definition is needed in
clinical practice to identify a clinically relevant worsening which will guide
us make treatment decisions. While the ACR core variables are primarily
physician based criteria, patient reported variables could have a significant
role in helping patients identify worsening early and seek medical attention
sooner .Our aims were to 1) Examine the feasibility of using Patient Reported
Outcomes (PROs) and ACR core set variables to define flare in children with JIA
and 2) Examine the concordance between the two definitions
Methods: We studied children in the Research in Arthritis in
Canadian Children emphasizing outcomes (ReACCh-Out) prospective cohort. Data
were collected during routine clinical practice for newly diagnosed patients at
16 pediatric rheumatology centres enrolled between 2005 and 2010. ACR core set
variables and patient reported variables were collected at 0, 6, 12, 18, 24,
36, 48 and 60 months after enrolment. The PROs included Pain visual analogue
scale, functional status measured by the Childhood Health Assessment
Questionnaire (CHAQ) and duration of morning stiffness. Flare was defined as:
1) PROs flare: at least 30% worsening in 2/3 PROs with minimum duration for
stiffness of 30 minutes; 2) ACR Core Set flare: worsening of at least 3/6 ACR core
variables by at least 30% without concomitant improvement of more than one
variable by ≥ 30%. Flare status was assessed for each patient visit after
the subject attained clinically inactive disease. Concordance between the two
flare definitions was assessed with the Kappa statistic. The risk of first flare
was estimated by Kaplan-Meier survival analysis.
Results: A total of 1146 patients were included in the study
with a median follow up of 24 months after inactive disease. Of the total 6177
study visits, 2358 visits occurred after patients had attained inactive
disease. Imputation was required for missing data in 42 % of visits for ACR
core variables and 35 % for PROs. After imputation the definition for flare
was fulfilled in 478 (20.2%) visits using ACR core variables and in 366 (15.5%)
visits using PRO variables. In 231 visits flare was identified by both
definitions. The overall concordance was 83.8% with kappa value of 0.45
suggesting moderate agreement (p =0.00001). Applying minimum cut-offs for ACR core
variables, as done in randomized trials of polyarticular course JIA, only 278
visits would fulfill the criteria. The Kaplan Meier curves are presented in
the figure.
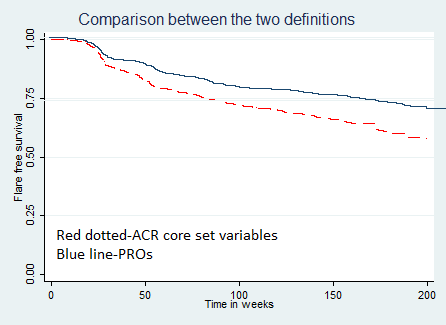
Conclusion: A flare definition based on PROs had moderate
concordance with the one based on ACR core set variables. It tended to
underestimate the risk of flare. The feasibility of using both the definitions
to define flare in this routine practice-based cohort was limited by missing
data requiring imputation and by study visits scheduled at set intervals.
To cite this abstract in AMA style:
Shivamurthy V, Levy DM, Boire G, Watanabe Duffy KN, Stringer E, Scuccimarri R, Yeung RSM, Huber AM, Oen K, Shiff N, Tucker LB, Berard R, Morishita K, Duffy CM, Guzman J. Flare Definitions for Juvenile Idiopathic Arthritis (JIA) Based on ACR Core Set Variables and Patient Reported Outcomes: Results from the Research in Arthritis in Canadian Children-Emphasizing Outcomes Prospective Cohort [abstract]. Arthritis Rheumatol. 2015; 67 (suppl 10). https://acrabstracts.org/abstract/flare-definitions-for-juvenile-idiopathic-arthritis-jia-based-on-acr-core-set-variables-and-patient-reported-outcomes-results-from-the-research-in-arthritis-in-canadian-children-emphasizing-outcome/. Accessed .« Back to 2015 ACR/ARHP Annual Meeting
ACR Meeting Abstracts - https://acrabstracts.org/abstract/flare-definitions-for-juvenile-idiopathic-arthritis-jia-based-on-acr-core-set-variables-and-patient-reported-outcomes-results-from-the-research-in-arthritis-in-canadian-children-emphasizing-outcome/