Session Information
Session Type: Abstract Submissions (ACR)
Background/Purpose:
Macrophage activation syndrome (MAS) is a life-threatening inflammatory complication of pediatric systemic lupus erythematosus (pSLE). There are few reports of the presentation, treatment and outcome of MAS in pSLE. Our objective is to describe the presentation and treatment of pSLE-MAS patients seen at a single tertiary centre.
Methods:
Our retrospective review included all patients seen at the Hospital for Sick Children, Toronto, diagnosed with pSLE (³ 4/11 ACR classification criteria) and MAS (by Pediatric Reumatologist expert opinion) between January 2002 and December 2012. We collected data on: 1) Demographics: Sex, ethnicity, age of diagnoses; 2) MAS clinical features (fever, hepatosplenomegaly, lymphadenopathy, hemorrhages, CNS involvement); 3) SLE ACR classification criteria; 3) Additional laboratory, pathological and genetic parameters including autoantibodies and bone marrow aspiration (BMA); 4) Treatment; 5) Frequency of hospitalization, PICU admission and death.
Results:
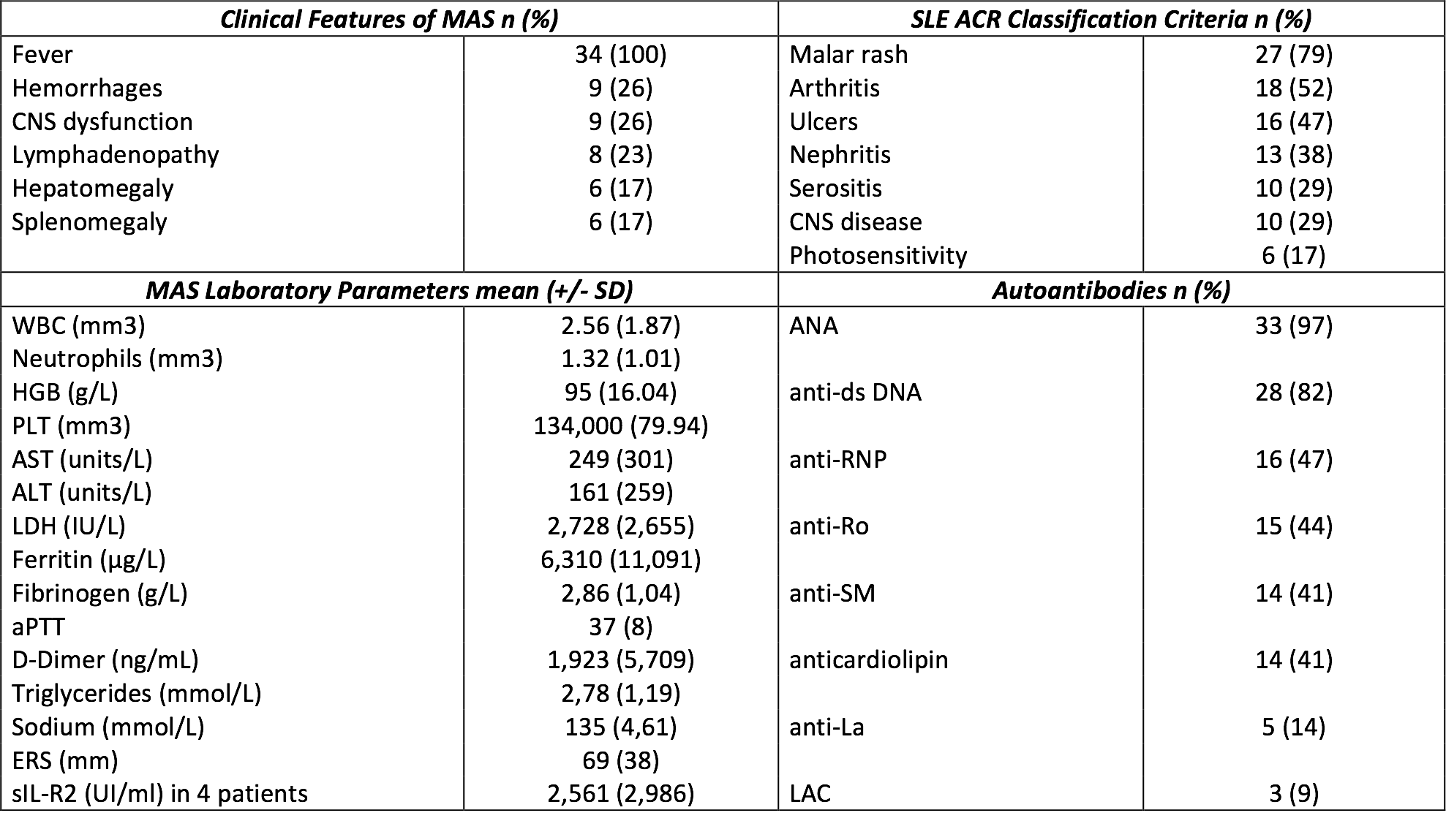
We identified 34 patients diagnosed with pSLE and MAS. The majority were female (70%). The most common SLE features were malar rash, arthritis and anti-dsDNA antibodies (Table). Mean age at SLE diagnosis was 13.4 years (SD: 3.0), the average interval between SLE and MAS diagnosis was 1.5 months (SD: 0.54), with the majority (76%) of patients diagnosed with MAS concomitantly with their SLE diagnosis. 4 patients had documented concomitant infections: 2 bacterial, 1 EBV and 1 HSV1.
All patients had fever (Table). 6/23 patients (26%) who underwent BMA demonstrated hemophagocytosis. Targeted gene sequencing of HLH genes perforin and syntaxin 11 was performed in 5 patients with the only abnormality a silent heterozygous polymorphism in perforin coding region detected in one patient. All patients were treated with corticosteroids with the majority (59%) receiving IV pulse of methylprednisolone (average 3 pulses/patient). Concomitant medications: IVIG in 59%, calcineurin inhibitor in 32%, and etoposide in 6%. All the patients required hospital admission, 6 required PICU admission and there were no deaths from MAS.
Conclusion:
To our knowledge this is the largest cohort of patients with diagnosis of MAS in pSLE reported in a single center. We observed that MAS is most likely to develop concomitantly with pSLE diagnosis. The majority of the patients were successfully treated with corticosteroids and IVIG with complete recovery in all.
Table: Clinical and Laboratory characteristics:
Disclosure:
R. E. Borgia,
None;
M. Gerstein,
None;
D. M. Levy,
None;
E. D. Silverman,
None;
L. T. Hiraki,
None.
« Back to 2014 ACR/ARHP Annual Meeting
ACR Meeting Abstracts - https://acrabstracts.org/abstract/features-treatment-and-outcome-of-macrophage-activation-syndrome-in-pediatric-systemic-lupus-erythematosus/