Session Information
Date: Tuesday, November 10, 2015
Title: Systemic Sclerosis, Fibrosing Syndromes and Raynaud's - Clinical Aspects and Therapeutics Poster III
Session Type: ACR Poster Session C
Session Time: 9:00AM-11:00AM
Background/Purpose:
Exercise
intolerance is common in patients with connective tissue disease (CTD) and may
be related to pulmonary hypertension (PH). However, determining the exact etiology
of the exercise limitation in these patients is challenging due to the
multiorgan involvement of CTDs. The invasive cardiopulmonary exercise testing (iCPET)
combines the non-invasive evaluation of an incremental symptom-limited cycling CPET
with simultaneous pulmonary and radial artery-derived invasive hemodynamics measurements,
and therefore differentiate among cardiovascular, respiratory, metabolic and
peripheral limitations to exercise. In the current study, we evaluated patients
with CTD and exertional intolerance (with or without interstitial lung disease,
ILD) who underwent iCPET. Our aim was to determine the relative contributions
of central cardiac and peripheral mechanisms underlying exertional intolerance
in CTD patients. We hypothesized that CTD without ILD would have multifactorial
reasons for exertional intolerance, beyond PH.
Methods:
683
clinically indicated iCPETs performed at Brigham and Women’s Hospital between
2011-2015 were evaluated. Based on established diagnostic criteria 50 patients had
confirmed CTD (18 SSc, 15 RA, 4 UCTD, 3 SLE, 3 antisynthetase syndrome, 2
CREST, 2 MCTD, 1 psoriatic arthritis, 1 Sjögren’s, 1 Still’s). ILD was defined
by the presence of fibrosis on CT scans of the lungs and a forced vital
capacity < 70% predicted.
Results:
From
the 50 patients evaluated, 15 had CTD-ILD, of which 14 (93%) had PH. Among the
35 patients without ILD, 23 (66%) had a reduced aerobic capacity defined by maximum
oxygen uptake (VO2MAX) < 80% predicted. Out of these 23 patients,
10 (43%) had PH and 13 (57%) had a non-PH related exercise diagnosis, most
commonly a peripheral limitation to exercise (10 of 13). Subgroup analysis of systemic
sclerosis (SSc) patients revealed 10 of 18 (56%) with ILD, and PH was the most
common diagnosis. SSc patients without ILD and a reduced VO2MAX were
more likely to have a peripheral limitation to exercise (5 of 7, Figure 1). VO2MAX
was 62±15% predicted for the CTD-ILD group, 60±16% for CTD without ILD with
PH-related limitation to exercise, and 63±12% for CTD without ILD and a non-PH
disease. There were no significant differences regarding VO2MAX among
these three groups (p>0.05).
Conclusion:
With
direct measures from iCPET, we conclude that while CTD-ILD patients are more
likely to present a PH-related limitation to exercise, CTD patients without ILD
have a higher prevalence of peripheral limitation manifested by impaired
systemic O2 extraction. We speculate the latter may be related to
skeletal muscle mitochondrial dysfunction and/or peripheral microvascular dysfunction.
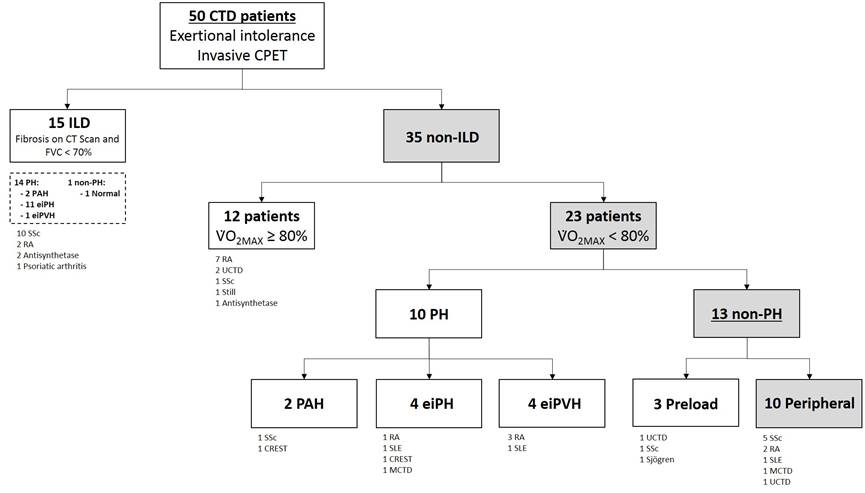 Figure
Figure
1.
To cite this abstract in AMA style:
Oliveira R, Systrom D, Tracy J, Karin A, Waxman A, Dellaripa P, Hoover P. Exercise Intolerance Evaluated By Invasive Cardiopulmonary Exercise Testing in Connective Tissue Disease: Beyond Pulmonary Hypertension [abstract]. Arthritis Rheumatol. 2015; 67 (suppl 10). https://acrabstracts.org/abstract/exercise-intolerance-evaluated-by-invasive-cardiopulmonary-exercise-testing-in-connective-tissue-disease-beyond-pulmonary-hypertension/. Accessed .« Back to 2015 ACR/ARHP Annual Meeting
ACR Meeting Abstracts - https://acrabstracts.org/abstract/exercise-intolerance-evaluated-by-invasive-cardiopulmonary-exercise-testing-in-connective-tissue-disease-beyond-pulmonary-hypertension/