Session Information
Session Type: Poster Session (Monday)
Session Time: 9:00AM-11:00AM
Background/Purpose: Anti-neutrophil cytoplasmic antibody (ANCA) associated vasculitis (AAV) is the most prevalent adult vasculitis and is associated with significant inflammatory burden; chest computed tomography (CT) is frequently obtained as part of the diagnostic work up and prognosis. Coronary calcium score (CCS) is a non-invasive modality used to evaluate the presence of coronary arterial calcium (CAC). Visual assessment of CAC via previously validated ordinal scoring in routine non-gated chest CT accurately predicts CCS (in Agatston units) from electrocardiogram-gated CT. Studies have demonstrated increased CCS/CAC burden in rheumatoid arthritis and systemic lupus erythematosus, but none have studied vasculitides, specifically AAVs: granulomatosis with polyangiitis (GPA), eosinophilic granulomatosis with polyangiitis (EGPA), and microscopic polyangiitis (MPA). We evaluated the cardiovascular burden in AAVs through visual assessment of CAC, compared to matched controls.
Methods: In a single tertiary care center we performed a retrospective chart review (2006-2018) of all adults with GPA, MPA, and EGPA (identified by ICD-9 and ICD-10 code) who had routine non-gated chest CT within 1 year before, or any time after diagnosis, and cholesterol profile within 5 years of diagnosis. Exclusion criteria included a history of coronary artery disease (CAD), peripheral arterial disease, or stroke. Abstracted data included: demographics, AAVs characteristics including the Birmingham vasculitis activity score (BVAS), and CAD risk factors. One thoracic radiologist blindly reviewed the chest CTs of AAVs and control patients matched by age (within 5 years), sex, race, body mass index (BMI, within 3 units), and same year of chest CT. CAC was scored ordinally: 0 = none, 1 = mild, 2 = moderate, and 3 = severe, in each of the main four coronary arteries; total scores ranged 0-12. All chest CTs were done without intravenous contrast.
Results: We identified 61 AAV patients and 61 controls (Table 1). For the AAV group: disease duration (mean ± SD) until CT scan was 37.2 ± 25.8 months, subjects were mostly white (88.5 %), and female (60.7%); BVAS was able to be calculated within 6 months of CT scan in 53 (87%) of subjects with a mean score of 6. Creatinine was significantly higher in the AAV group (P = 0.028). The mean CAC scores (AAV: 2.18 ± 2.46; control: 1.46 ± 1.80; P = 0.089) and prevalence of CAC (AAV: 60.7%, control: 54.1%; P = 0.464) in AAVs were not significantly different compared to controls (Table 2). The prevalence of CAC in AAVs, even when adjusted for CAD risks, was not significantly different compared to controls. 34 of the AAV patients (64%) had a BVAS > 0, but the CAC score was comparable to controls (P = 0.26). Longer disease duration was not associated with higher CAC score or prevalence (Table 3).
Conclusion: CAC interpreted through ordinal scoring is similar in patients with GPA, MPA, or EGPA, compared to control group. Though CAC score and prevalence were higher in the vasculitis group, they did not reach statistical significance (likely due to small sample size and retrospective nature of our study). Controlled prospective studies are needed to best analyze the cardiovascular risk and utility of CAC assessment in AAV.

Table 1. Clinical characteristics
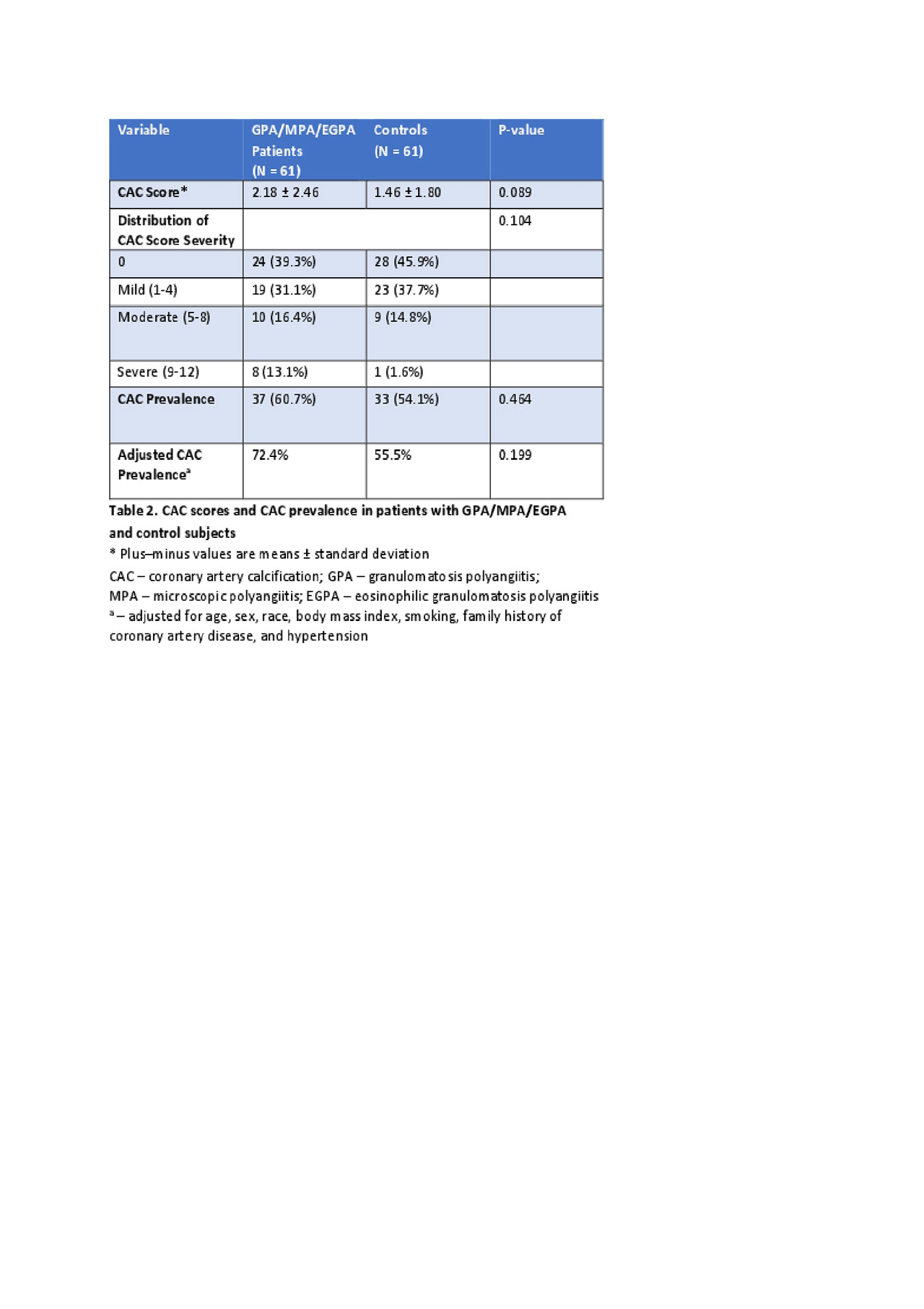
Table 2. CAC score and prevalance

Table 3. CAC disease duration
To cite this abstract in AMA style:
Farshad S, Halalau A, Al-Katib S, George J, Schiopu E. Evaluation of Subclinical Coronary Atherosclerosis in ANCA-associated Small Vessel Vasculitides (AAVs) Compared to Matched Controls Through Visual Assessment of Coronary Arterial Calcium (CAC) Score Using Non-Gated Chest Computed Tomography (CT) [abstract]. Arthritis Rheumatol. 2019; 71 (suppl 10). https://acrabstracts.org/abstract/evaluation-of-subclinical-coronary-atherosclerosis-in-anca-associated-small-vessel-vasculitides-aavs-compared-to-matched-controls-through-visual-assessment-of-coronary-arterial-calcium-cac-score-u/. Accessed .« Back to 2019 ACR/ARP Annual Meeting
ACR Meeting Abstracts - https://acrabstracts.org/abstract/evaluation-of-subclinical-coronary-atherosclerosis-in-anca-associated-small-vessel-vasculitides-aavs-compared-to-matched-controls-through-visual-assessment-of-coronary-arterial-calcium-cac-score-u/