Session Information
Date: Tuesday, October 23, 2018
Title: Pediatric Rheumatology – Clinical Poster III: Juvenile Idiopathic Arthritis and Uveitis
Session Type: ACR Poster Session C
Session Time: 9:00AM-11:00AM
Background/Purpose: It is widely accepted that the treatment goal for juvenile idiopathic arthritis (JIA) is remission. PR-COIN, a quality improvement collaborative comprised of pediatric rheumatology centers, measures JIA disease activity in patients using the ACR provisional criteria for Clinical Inactive Disease (CID). Significant center-level differences in the percentage of patients in CID have been observed across the network. The objective of the current study was to identify differences between patient-level variables in centers with higher vs lower percentage of patients in CID, although we hypothesize that these differences are primarily driven by center-level factors rather than patient case-mix.
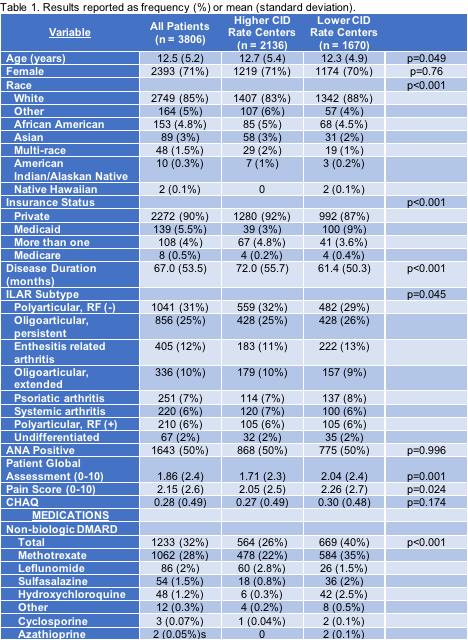
Methods: This study used cross-sectional data provided by PR-COIN that was collected by PR-COIN centers in the ACR Rheumatology Clinical Registry between March 2015 and May 2016. For each patient, variables from the most recent visit were recorded and included age, gender, race, insurance status, duration of diagnosis, ILAR subtype, ANA status, patient global assessment, pain score, Childhood Health Assessment Questionnaire (CHAQ) score, and current medication use. Patients were grouped into two categories based on the percentage of patients in CID at their center (above or below the network average). Statistical analyses were performed using R software, including descriptive analyses and two-group comparisons with chi-square for categorical variables and independent t-tests for continuous variables. Missing data were excluded with each analysis.
Results: There were 3806 patients eligible for analysis from 15 centers. The median center-level rate of CID was estimated at 45.6% with a range from 26.1% to 57.9%. The 7 centers categorized as “higher performing” contained 2136 patients and the 8 centers categorized as “lower performing” contained 1670 patients. Comparing patients from the “higher” vs. patients from the “lower” centers, key significant differences included race, insurance status, disease duration, patient global assessment, pain score, and current use of non-biologic DMARDs, biologic DMARDs, TNF inhibitors, NSAIDs, and glucocorticoids (see Table 1).
Conclusion: By leveraging the framework of a quality improvement learning network such as PR-COIN, we are able to determine predictors of disease activity outcomes using data from clinical practice. This analysis demonstrates preliminary differences in patient characteristics between patients at centers with higher vs lower rates of CID; more advanced modeling is needed to further evaluate these findings. Future directions include development and implementation of interventions to address identified predictors, which can then be tested and spread through the multi-center infrastructure of PR-COIN. This work has the potential to directly impact care delivery and improve outcomes for JIA.
To cite this abstract in AMA style:
Smitherman EA, Huang B, Laxer RM, Bingham CA, Yildirim-Toruner C, Gottlieb B, Weiss J, Lee T, Vora SS, Burnham J, Harris J, Olson JC, Gilbert M, Batthish M, Shishov M, Fleck D, Morgan E. Evaluating Disease Activity Outcomes for Juvenile Idiopathic Arthritis across the Pediatric Rheumatology Care and Outcomes Improvement Network (PR-COIN) [abstract]. Arthritis Rheumatol. 2018; 70 (suppl 9). https://acrabstracts.org/abstract/evaluating-disease-activity-outcomes-for-juvenile-idiopathic-arthritis-across-the-pediatric-rheumatology-care-and-outcomes-improvement-network-pr-coin/. Accessed .« Back to 2018 ACR/ARHP Annual Meeting
ACR Meeting Abstracts - https://acrabstracts.org/abstract/evaluating-disease-activity-outcomes-for-juvenile-idiopathic-arthritis-across-the-pediatric-rheumatology-care-and-outcomes-improvement-network-pr-coin/