Session Information
Date: Monday, November 9, 2015
Session Type: ACR Poster Session B
Session Time: 9:00AM-11:00AM
Epidemiology of Sarcoidosis
1976-2013: A Population-Based Study
Background/Purpose: The epidemiology of sarcoidosis is
not well-described. Only coding-based studies with point estimates over
relatively short periods, without detailed case information or verification
based on individual medical record review have been reported. This study aimed
to characterize the epidemiology of sarcoidosis, with emphasis on annual
incidence and mortality, from 1976 to 2013.
Methods: An inception cohort of patients with incident sarcoidosis in 1976-2013
in a geographically well-defined population was identified based on comprehensive
individual medical record review. Inclusion required physician diagnosis
supported by histopathology and radiologic features of intrathoracic sarcoidosis,
compatible clinical presentation, and exclusion of other granulomatous diseases.
Tissue samples are considered positive if they demonstrate non-caseating
granuloma without evidence of acid-fast bacilli or fungi. The only exception to the requirement of histopathological
confirmation was stage I pulmonary sarcoidosis that required only radiographic
evidence of symmetric bilateral hilar adenopathy. Isolated granulomatous
disease of the skin without other features of sarcoidosis was not considered. Incidence
rates were age and sex adjusted to the US white 2010 population.
Results: In 1976-2013, 345 incident cases of
sarcoidosis were identified (mean age 45.6 years and 50.4% female). The annual
incidence of sarcoidosis was 10.8 per 100,000 population (11.0 per 100,000
population in female and 10.5 per 100,000 population in male). The peak
incidence was observed in those who were 35 to 64 years old. The numbers of
minorities were too low to establish separate estimates by self-assigned
ethnicity. Significant changes of incidence over time were not observed (Figure
1).
97% of cases had intra-thoracic involvement (87% intra-thoracic
lymphadenopathy and 50% pulmonary parenchymal infiltration). Only 43% of
patients had respiratory symptoms. The most common extra-thoracic
manifestations were skin rash, arthralgia, ophthalmologic and hepatic
involvement (18%, 14%, 7% and 6%, respectively). Isolated extrapulmonary sarcoidosis
was diagnosed in 10 (3% of patients).
During median follow-up of 12.2 years (5002 total
person-years), 50 patients died. The overall mortality of patients with
sarcoidosis was not different from general population (standardized mortality
ratio: 0.85; 95% CI, 0.63-1.13). Significant changes of mortality over time
were not observed as well.
Conclusion: Sarcoidosis occurred in about 11 persons per 100,000 per
year. Most of the patients had intra-thoracic involvement, although less than
half had respiratory symptoms. Overall mortality was not different from general
population.
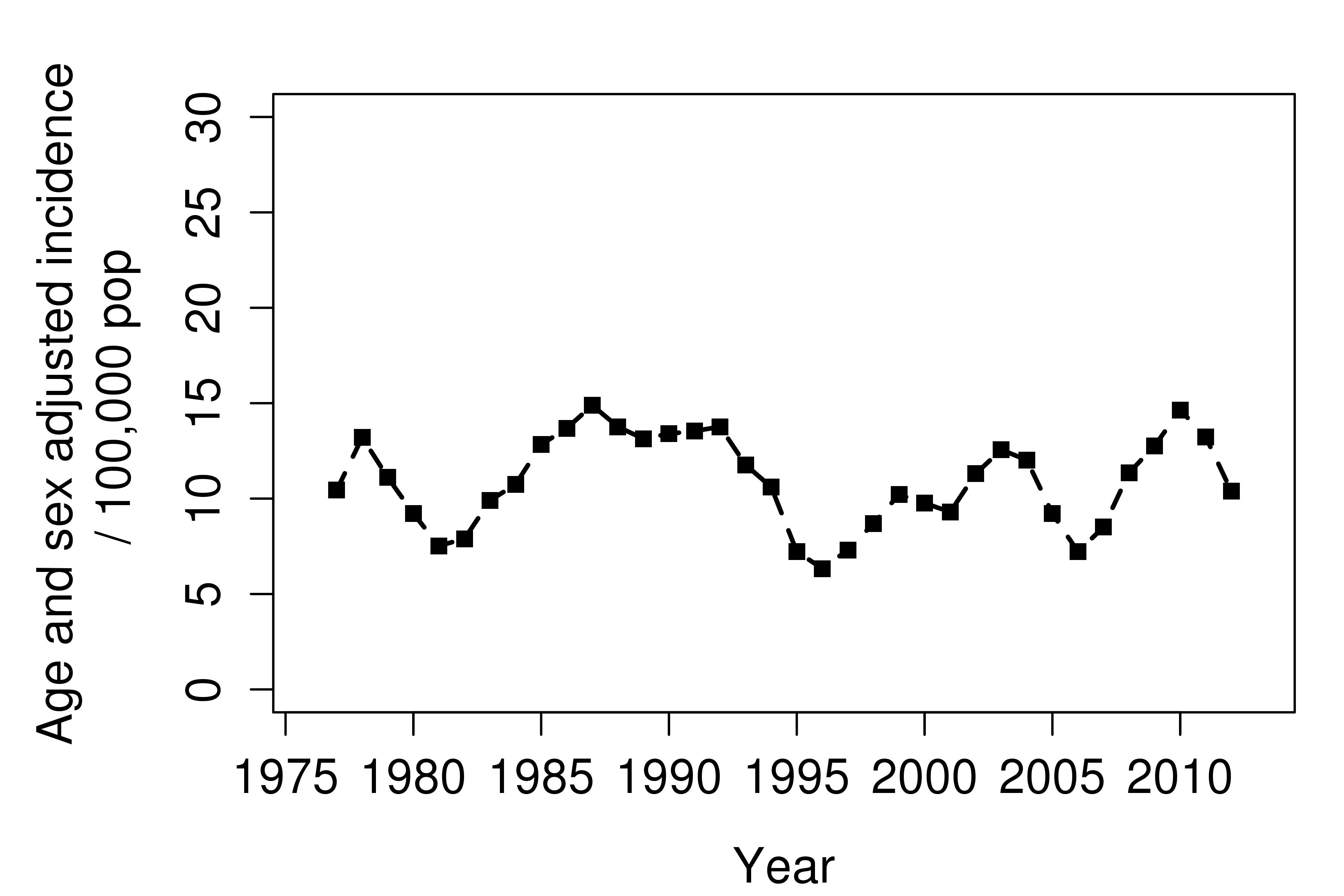
Figure 1. Trends in incidence of sarcoidosis 1976-2013
overall
To cite this abstract in AMA style:
Ungprasert P, Carmona Porquera EM, Utz JP, Ryu JH, Crowson CS, Matteson EL. Epidemiology of Sarcoidosis 1976-2013: A Population-Based Study [abstract]. Arthritis Rheumatol. 2015; 67 (suppl 10). https://acrabstracts.org/abstract/epidemiology-of-sarcoidosis-1976-2013-a-population-based-study/. Accessed .« Back to 2015 ACR/ARHP Annual Meeting
ACR Meeting Abstracts - https://acrabstracts.org/abstract/epidemiology-of-sarcoidosis-1976-2013-a-population-based-study/