Session Information
Date: Monday, November 9, 2015
Session Type: ACR Poster Session B
Session Time: 9:00AM-11:00AM
Background/Purpose:
Giant cell arteritis (GCA) is the
most common systemic vasculitis in persons older than 50 years. The highest
incidence rates of the disease have been reported in the Scandinavian
countries. However, the epidemiology is changing as the elderly population is
increasing. The aim of this study was to investigate the epidemiology of GCA in
an expected high-incidence region over time.
Methods:
This is a
retrospective cohort study of patients diagnosed with GCA in the hospitals of
Bergen Health Area (Helse Bergen) during 1972-2012. The International
Classification of Diseases (ICD)-coding system was used to identify patients
from hospital records, ICD-8 (446.4) for 1972-1987, ICD-9 (446.5) for 1987-1998
and ICD-10 (M31.5-6) for 1999-2012. The diagnosis was verified according to ACR
classification criteria by review of patient charts. The 820 patients who
satisfied these criteria were selected for initial analyses. Long term patient
outcomes were documented by review of patient charts from time of diagnosis
until time of death or end of study (31 Dec 2012). Information on time and
cause of death was collected from the Norwegian Cause of Death Registry. Incidence was calculated by using population
data for Hordaland County from Statistics Norway.
Results:
Among 820 identified GCA patients
there were 585 females (mean age 73.4 years, SD 8) and 235 males (mean age
71.7, SD 9). Five-hundred twenty-eight patients (64 %) had a positive temporal
artery biopsy and 206 patients (25 %) had a negative biopsy. For the remaining
86 patients (11 %) biopsy was not performed or biopsy results were
inconclusively or insufficiently reported. Patient characteristics and outcomes are presented in table 1.
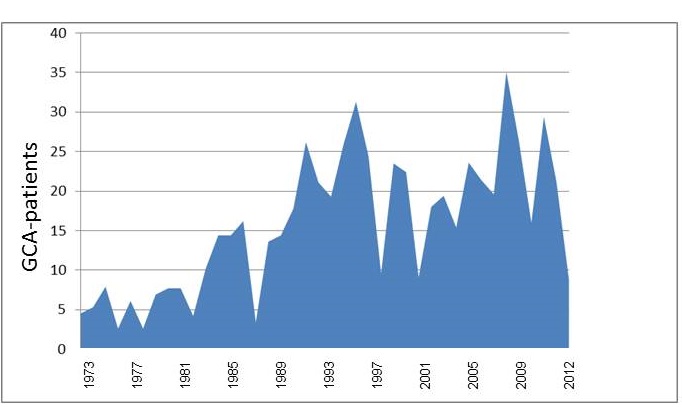
The average annual incidence rate
for GCA was 15.7 per 100 000 > 50 years (females 20.4 and males 9.9). There were large
fluctuations in incidence according to year of diagnosis with a tendency of
progressive increase. The highest annual incidence rate observed was 35.1 in 2007. The lowest annual incidence rate was 2.6 in 1976 and 1978. Yearly distribution of
incidence rates is displayed in figure 1.
Four-hundred forty-three patients
(54 %) of our cohort died during the follow-up period.
Conclusion:
An increasing cumulative incidence
throughout the period 1972-2012 was observed in our study. Higher awareness of
GCA among clinicians could be an explanation. This interesting finding warrants
further investigation.
|
Table 1. Patient characteristics and outcomes |
||||
|
|
|
Overall n=820 |
Female n=585 |
Male n=236 |
|
Mean age at onset of GCA (SD) |
|
72.9 (8.7) |
73.4 (8.4) |
71.7 (9.3) |
|
|
|
|
|
|
|
ACR criteria fulfilled (%) |
|
820 (100) |
|
|
|
Age ≥ 50 at disease onset (%) |
|
816 (99.5) |
583 (99.7) |
233 (99.1) |
|
New onset headache (%) |
|
592 (72.2) |
418 (71.5) |
174 (74.0) |
|
Temporal artery tenderness (%) |
|
378 (46.1) |
265 (45.3) |
113 (48.1) |
|
Decreased temporal pulse(%) |
|
230 (28) |
170 (29.1) |
60 (25.5) |
|
ESR ≥ 50 (%) |
|
740 (90.2) |
525 (89.7) |
215 (91.5) |
|
Biopsy showing vasculitis (%) |
|
528(64.4) |
378 (64.6) |
150 (63.8) |
|
Giant cells in biopsy (%) |
|
243 (29.6) |
185 (31.6) |
58 (24.7) |
|
|
|
|
|
|
|
Mean ESR (SD) n=810 |
|
84.1 (27.6) |
83.7 (27.9) |
85.1 (27.0) |
|
Mean CRP (SD) n=626 |
|
90.3 (63.4) |
87.5 (62.3) |
97.7 (65.2) |
|
|
|
|
|
|
|
Jaw claudication (%) |
|
181 (22.1) |
134 (22.9) |
47 (20) |
|
Polymyalgia Rheumatica (%) |
|
246 (30) |
195 (33.3) |
51 (21.7) |
|
Peripheral Arthritis (%) |
|
35 (4.3) |
25 (4.3) |
10 (4.3) |
|
Visual disturbance (%) |
|
149 (18.2) |
106 (18.1) |
43 (18.3) |
|
Blindness one or both eyes (%) |
|
33 (4) |
24 (4.1) |
9 (3.8) |
|
Scalp necrosis (%) |
|
6 (0.7) |
4 (0.7) |
2 (0.9) |
|
|
|
|
|
|
|
Number of deaths 1972-2012 (%) |
|
443 (54) |
311 (53.2) |
132 (56.2) |
|
|
|
|
|
|
Figure 1: Annual
incidence rate of GCA per 100 000 persons age > 50
years
To cite this abstract in AMA style:
Brekke LK, Diamantopoulos AP, Esperø EL, Fevang BT, Brun JG, Gjesdal CG. Epidemiology of GCA in Bergen (Western Norway) 1972-2012 [abstract]. Arthritis Rheumatol. 2015; 67 (suppl 10). https://acrabstracts.org/abstract/epidemiology-of-gca-in-bergen-western-norway-1972-2012/. Accessed .« Back to 2015 ACR/ARHP Annual Meeting
ACR Meeting Abstracts - https://acrabstracts.org/abstract/epidemiology-of-gca-in-bergen-western-norway-1972-2012/