Session Information
Session Type: ACR Poster Session A
Session Time: 9:00AM-11:00AM
Enthesitis in Juvenile Idiopathic Arthritis (JIA)
Background/Purpose: The characteristics of enthesitis, a feature in some children with juvenile idiopathic arthritis (JIA), t has not been well described in large prospective inception cohorts. We used data from a Canadian cohort to describe the characteristics of patients with enthesitis, the sites most commonly affected, and the temporal changes in the number of sites of enthesitis, relative to changes in active joint counts.
Methods: Children newly diagnosed with JIA at 16 Canadian centers from 2005 to 2010 were followed in the ReACCh-Out cohort for up to 5 years. For this analysis, all patients with >1 visit (n=1406) were included. The presence and location of enthesial tenderness on examination were recorded by pediatric rheumatologists in all children present at 0, 6, 12, 18, 24, 36, 48 and 60 months after enrolment. For this study, a child was said to have enthesitis if enthesial tenderness was present on >1 occasion and/or at >1 body site. The characteristics of patients with an without enthesitis were compared using univariate logistic regression on each characteristic. The number of tender enthesial sites was analyzed over time and compared to the number of active joint counts using linear mixed models for longitudinal data.
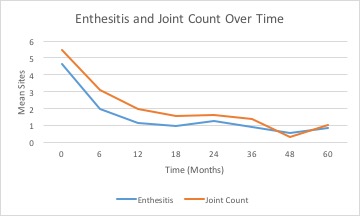
Results: A total of 219 patients (16% of the cohort) fulfilled our criteria for enthesitis; 8% fulfilled criteria at enrolment and 15% fulfilled criteria within 2 years. The most frequent sites of involvement were the calcaneal plantar insertion (39%), Achilles insertion (31%), and tibial tuberosity (30%). The characteristics of children with and without enthesitis are presented in Table 1. Children with enthesitis were older, more often male and 141 (64.4%) were categorized as enthesitis related arthritis; 57.1% had polyarticular involvement and 30% had sacroiliac involvement at some point during follow-up. The mean number of tender enthesial sites decreased dramatically over the follow-up period, roughly in parallel with the number of active joints (see Figure 1, p=0.16 for whole group). A mixed linear model analysis showed no significant difference in active joint counts over time in children with or without enthesitis (p=0.73).
Conclusion: The number of patients with enthesitis and their characteristics were generally as expected, except that over half the patients had polyarticular involvement. The number of tender enthesial sites and active joints decreased similarly over time in the enthesitis group, and the active joint counts decreased similarly over time in children with and without enthesitis. Table 1: Characteristics of Patients With Versus Without Enthesitis
| Characteristic |
Patients with Enthesitis |
Patients without Enthesitis |
OR (95% CI) |
| Number with Enthesitis |
219 (15.6%) |
1187 (84.4%) |
|
| Age of onset of JIA (Mean) |
10.7 yrs (SD 3.2 yrs) |
7.5 years (SD 4.6 yrs) |
1.21 (1.16 Ð 1.26) |
| Male Sex |
124 (56.6%) |
365 (30.8%) |
2.89 (2.15 Ð 3.88) |
| ANA Positive* |
51 (23.3%) |
563 (47.4%) |
0.33 (0.24 Ð 0.47) |
| HLA-B27 Present** |
70 (32.0%) |
75 (6.3%) |
4.58 (3.09 Ð 6.81) |
| JIA Subtype (Initial) |
|
|
|
| -ERA |
141 (64.4%) |
61 (5.1%) |
Reference |
| -Oligoarticular |
13 (5.9%) |
546 (46%) |
0.010 (0.006 Ð 0.02) |
| -Polyarticular RF Ðve |
17 (7.8%) |
256 (21.6%) |
0.029 (0.02 Ð 0.05) |
| -Polyarticular RF +ve |
4 (1.8%) |
53 (4.5%) |
0.033 (0.01 Ð 0.09) |
| -Systemic |
0 (0%) |
86 (7.25%) |
Cannot compute |
| -Psoriatic |
5 (2.3%) |
83 (7.0%) |
0.026 (0.01 Ð 0.067) |
| -Unclassified |
39 (17.8%) |
102 (8.6%) |
0.17 (0.1 Ð 0.27) |
| Uveitis (ever) |
21 (9.6%) |
198 (16.7%) |
0.53 (0.33 Ð 0.85) |
| Sacroiliitis (ever) |
66 (30.1%) |
43 (3.6%) |
11.5 (7.5 Ð 17.5) |
| Psoriasis (ever) |
57 (26.0%) |
273 (23.0%) |
1.18 (0.85 Ð 1.64) |
| Polyarticular involvement (ever) |
125 (57.1%) |
487 (41.0%) |
1.91 (1.43 Ð 2.56)
|
*ANA status unknown in 11.9% of the enthesitis group and 8.4% of the no enthesitis group **HLA-B27 status unknown in 26.5% of the enthesitis group and 56.0% of the no enthesitis group Figure 1: Mean Number of Tender Enthesial Sites and Active Joints in Children with Enthesitis
To cite this abstract in AMA style:
Rumsey DG, Guzman J, Rosenberg A, Huber A, Scuccimarri R, Eurich D. Enthesitis in Juvenile Idiopathic Arthritis (JIA) [abstract]. Arthritis Rheumatol. 2016; 68 (suppl 10). https://acrabstracts.org/abstract/enthesitis-in-juvenile-idiopathic-arthritis-jia/. Accessed .« Back to 2016 ACR/ARHP Annual Meeting
ACR Meeting Abstracts - https://acrabstracts.org/abstract/enthesitis-in-juvenile-idiopathic-arthritis-jia/