Session Information
Date: Tuesday, October 23, 2018
Title: Spondyloarthritis Including Psoriatic Arthritis – Clinical Poster III: Treatment
Session Type: ACR Poster Session C
Session Time: 9:00AM-11:00AM
Background/Purpose: VOYAGE 1 & 2 were the pivotal Ph3 GUS trials for plaque PsO.1,2 Here we compare efficacy of GUS vs PBO & adalimumab (ADA) on PsO involving scalp, nail & palmoplantar (palmoplantar pustular PsO excluded per protocol) PsO in subgrp of pts w/ self-reported PsA, given the association between these distinct PsO phenotypes & PsA.
Methods: VOYAGE 1(n=837) & VOYAGE 2(n=992) enrolled adult pts who had plaque PsO for ≥6 months, an Investigator Global Assessment (IGA) score ≥3, PASI score ≥12, ≥10% BSA involvement at baseline (BL), & were candidates for phototherapy or systemic treatment for PsO. Pts were randomized to GUS, PBO or ADA at BL, w/ PBO crossover to GUS at wk16. This post-hoc analysis used observed pooled efficacy data for scalp-specific (ss-IGA), Physician’s Global Assessment (PGA) of Hands &/or Feet (hf-PGA), fingernail PGA (f-PGA), & Nail Psoriasis Area & Severity Index (NAPSI) in subset of pts self-reporting PsA.
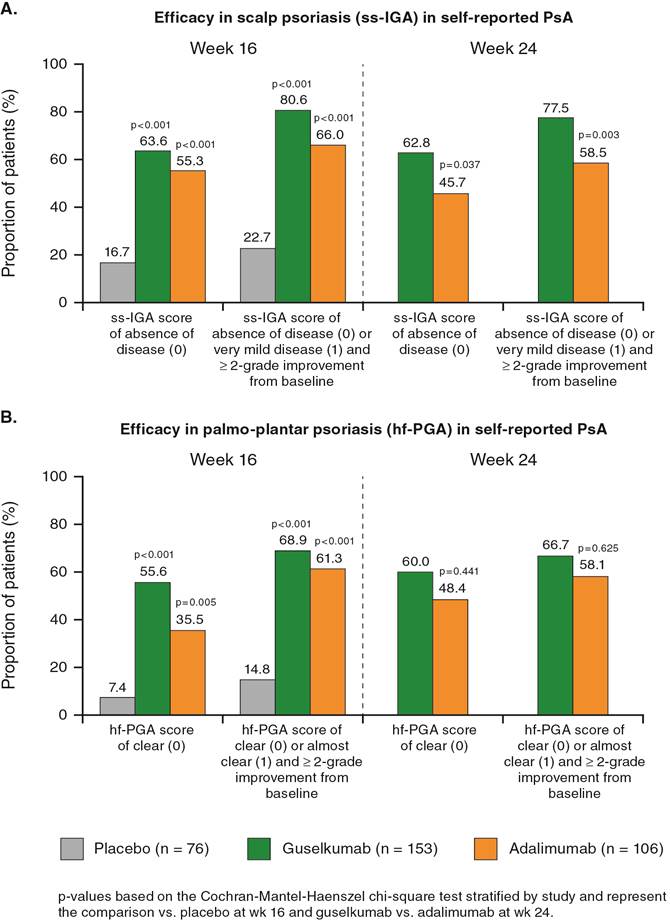
Results: In VOYAGE 1 & 2 combined, 335 (18.3%) PsO pts self-reported PsA (PBO 76, GUS 153, ADA 106). Baseline demographics were generally comparable across all 3 treatment grps, w/ history of methotrexate use: PBO 64.5%, GUS 70.6%, ADA 61.3%. A significantly greater proportion of GUS-treated pts achieved a ss-IGA score of 0/1 (absent/very mild) at wk16 vs PBO, & at wk24 vs ADA (Figure A). Significantly higher proportions of GUS-treated pts achieved a hf-PGA score of 0/1 (clear/almost clear) vs PBO at wk16 w/ numerically greater differences at wk24 vs ADA (Figure B).
At wk16, proportions of pts achieving a f-PGA score of 0/1 (clear/minimal) were 47.6% for GUS vs 17.0% for PBO (p<0.001). The proportions of pts achieving a f-PGA score of 0/1 for GUS vs ADA were comparable at wk16 (47.6% vs 46.4%) & wk24 (67.0% vs 60.9%), but were higher for GUS by wk48 (82.5% vs 57.5%, Table).
Mean (SD) % improvement from BL in NAPSI score was significantly higher for GUS vs PBO [39.5 (48.9) vs 6.5(47.5), p<0.001] at wk16 & was comparable for GUS vs ADA at wk24 [58.0 (51.3) vs 59.9 (40.4)]. By wk48, mean % improvement from BL in NAPSI score was higher for GUS vs ADA (70.8% vs 61.3%, Table).
Conclusion: GUS-treated PsO pts w/ self-reported PsA showed clinically meaningful improvements vs ADA in ss-IGA & hf-PGA scores at wks16 & 24. Although improvements in f-PGA & NAPSI were similar in pts treated w/ GUS vs. ADA at earlier timepoints, numerically greater differences were observed w/ GUS by wk48, likely requiring the additional duration to discriminate between treatments in this slow-growing cutaneous appendage.
1Blauvelt A, et al. J Am Acad Dermatol. 2017 Mar;76(3):405-417
2Reich K, et al J Am Acad Dermatol.2017 June;76(6): 1226
|
Table. Fingernail (f)-PGA score of clear (0) or minimal (1) in Psoriasis Patients with Self-Reported PsA at Wk 48* |
||
|
|
Guselkumab |
Adalimumab |
|
PsO Patients randomized at Week 0, n |
329 |
334 |
|
PsO Patients with Self-reported PsA, n |
64 |
62 |
|
Patients with f-PGA score >2 at baseline |
40 |
40 |
|
f-PGA score of clear (0) |
20 (50.0%) |
16 (40.0%) |
|
f-PGA score of clear (0) or minimal (1) |
33 (82.5%) |
23 (57.5%) |
|
Percent improvement from baseline in NAPSI Scores in Psoriasis Patients with Self-Reported PsA at Wk 48* |
||
|
|
Guselkumab |
Adalimumab |
|
PsO Patients randomized at Week 0, n |
825 |
582 |
|
PsO Patients with Self-reported PsA, n |
153 |
106 |
|
NAPSI (N) |
111 |
74 |
|
70.84 (40.49) |
61.25 (42.43) |
|
|
Median |
100.00 |
70.85 |
|
Range |
(-100.0; 100.0) |
(-50.0; 100.0) |
|
IQ range |
50.00; 100.00) |
(33.30; 100.00) |
|
*–Post-hoc analyses based on Voyage 1 only |
||
To cite this abstract in AMA style:
Orbai AM, Chakravarty SD, You Y, Kafka S, Karyekar CS, Merola JF. Efficacy of Guselkumab in Psoriasis Patients with Self-Reported Psoriatic Arthritis with Involvement of the Scalp, Nails, Hands, and Feet: A Pooled Analysis from 2 Pivotal Phase 3 Psoriasis Studies [abstract]. Arthritis Rheumatol. 2018; 70 (suppl 9). https://acrabstracts.org/abstract/efficacy-of-guselkumab-in-psoriasis-patients-with-self-reported-psoriatic-arthritis-with-involvement-of-the-scalp-nails-hands-and-feet-a-pooled-analysis-from-2-pivotal-phase-3-psoriasis-studies/. Accessed .« Back to 2018 ACR/ARHP Annual Meeting
ACR Meeting Abstracts - https://acrabstracts.org/abstract/efficacy-of-guselkumab-in-psoriasis-patients-with-self-reported-psoriatic-arthritis-with-involvement-of-the-scalp-nails-hands-and-feet-a-pooled-analysis-from-2-pivotal-phase-3-psoriasis-studies/