Session Information
Date: Sunday, November 13, 2016
Title: ARHP I: Exemplary Abstracts
Session Type: ARHP Concurrent Abstract Session
Session Time: 2:30PM-4:00PM
Background/Purpose: Much progress has been made in identifying risk factors for RA, but it is unclear whether individuals at risk for RA have knowledge of these factors. Potential educational interventions include reading materials, interactive web-based tools, and sessions with health educators. We assessed the effect of these educational interventions on RA risk factor knowledge among first-degree relatives (FDRs) of patients with RA using a randomized controlled trial.
Methods: We developed a web-based tool, the Personalized Risk Estimator for Rheumatoid Arthritis (PRE-RA), which collects data on an individual’s age, sex, family history, and risk-related behaviors; presents genetic and autoantibody results; displays relative risk and absolute risk of RA; and provides personalized education about RA risk. We randomly assigned FDRs without RA to 1 of 3 educational interventions: 1) Control group that received standard education about RA (n=80), 2) PRE-RA group that received personalized education via the web-based PRE-RA tool (n=80), and 3) PRE-RA Plus group that received PRE-RA and a one-on-one session with a health educator (n=78). We assessed RA knowledge at baseline and immediately, 6 weeks, and 6 months after education using the validated Illness Perception Questionnaire modified for RA. We calculated an RA knowledge score by summing the number of 8 RA risk factors that a subject agreed were related to RA. We used linear regression to compare RA knowledge scores from PRE-RA and PRE-RA Plus vs. controls at each time point adjusted for baseline score. We additionally evaluated the impact of the health educator in PRE-RA Plus vs. PRE-RA alone at each post-intervention time point as well as change in RA knowledge compared to baseline.
Results: Among 238 randomized FDRs at baseline, mean age was 45.6 years (SD 14.4), 76% were female, 88% were college educated, and mean RA knowledge score (possible range 0-8) was 4.3 (SD 1.9). At baseline, only 31% agreed smoking was a risk factor for RA, but this increased to 77% at 6 months after PRE-RA (p<0.001). Those who received PRE-RA or PRE-RA Plus had higher mean RA knowledge scores immediately (7.1 [SD 1.0]) and 6 months (6.3 [SD 1.6]) after personalized education compared to controls (immediate 5.3 [SD 1.7] and 6 months 4.8 [SD 2.0); p<0.001, Figure). Compared to only the PRE-RA tool, those who also met with a health educator had similar RA knowledge 6 months after education (improvement of 1.7 [SD 1.8] for PRE-RA; 2.4 [SD 1.9] for PRE-RA Plus, p=0.16).
Conclusion: Despite being both familiar with and at increased risk for RA, FDRs had low baseline knowledge about RA risk factors. We created an interactive, web-based personalized tool that educated FDRs about RA, and this increased knowledge persisted for 6 months. While there may be some additional benefit by also using a health educator, the PRE-RA tool alone is an effective method to educate individuals about RA risk factors to encourage positive health behaviors. 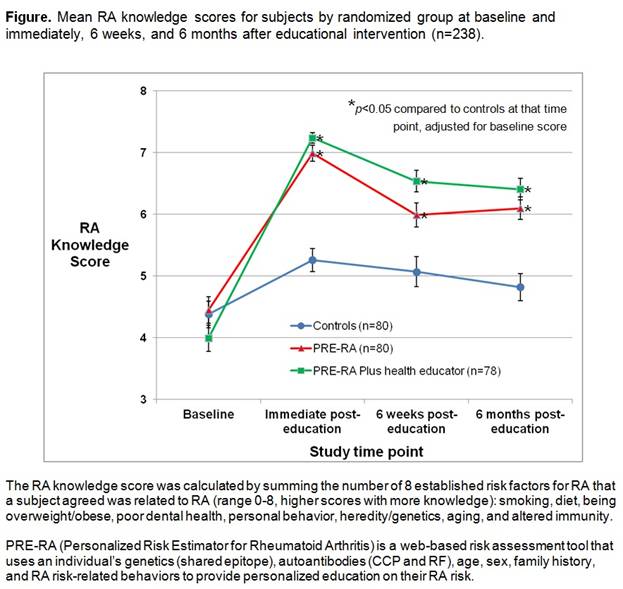
To cite this abstract in AMA style:
Prado MG, Miller Kroouze R, Yu Z, Iversen MD, Triedman NA, Kalia SS, Deane KD, Costenbader KH, Lu B, Green RC, Karlson EW, Sparks JA. Effectiveness of a Web-Based Personalized Rheumatoid Arthritis Risk Tool with or without a Health Educator for Knowledge of RA Risk Factors [abstract]. Arthritis Rheumatol. 2016; 68 (suppl 10). https://acrabstracts.org/abstract/effectiveness-of-a-web-based-personalized-rheumatoid-arthritis-risk-tool-with-or-without-a-health-educator-for-knowledge-of-ra-risk-factors/. Accessed .« Back to 2016 ACR/ARHP Annual Meeting
ACR Meeting Abstracts - https://acrabstracts.org/abstract/effectiveness-of-a-web-based-personalized-rheumatoid-arthritis-risk-tool-with-or-without-a-health-educator-for-knowledge-of-ra-risk-factors/