Session Information
Date: Tuesday, November 15, 2016
Title: Systemic Lupus Erythematosus – Clinical Aspects and Treatment - Poster III: Biomarkers and Nephritis
Session Type: ACR Poster Session C
Session Time: 9:00AM-11:00AM
Background/Purpose:
Proteinuria is the most common manifestation of lupus nephritis (LN) and it is an independent prognostic factor of long term outcomes. Recovery from proteinuria takes time with 52% of patients achieving complete proteinuria remission (CR) by 2 years from diagnosis of LN. We aimed to evaluate the effect of Complete Recovery (CR), Partial Recovery (PR), and No Recovery (NR) at 2 years from diagnosis of LN on long term outcomes.Methods:
Patients are followed at the Lupus Clinic at 2-6 month intervals according to a standard protocol which includes a complete history, physical examination and laboratory evaluation. Patients with LN (defined as proteinuria in a 24-hour urine sample [24H-P] > 0.5 g/day) attending the Lupus Center from 1970-2015 were included. At 2 years from diagnosis of LN, patients were divided in 3 groups (CR, PR, NR) based on 24H-P, and long-term outcomes were studied up to 15 years or last visit available. CR was defined as normal 24H-P (≤ 0.5 g/day), PR was defined as a reduction ≥ 50% in baseline 24H-P without achieving CR and NR was defined as a reduction < 50% 24H-P compared to baseline. Long term outcomes: 1-Renal outcomes (low [eGFR]: < 15 mL/min, end-stage renal disease requiring dialysis or transplantation [ESRD], and a Composite Renal Outcome [low eGFR or ESRD]); 2-Cardio-Vascular (CV) outcomes (angina or myocardial infarction); 3- Damage (SLICC/ACR Damage Index [SDI] ≥ 1); and 4- Death. Non-parametric tests (Log-rank tests) were applied to describe the effect of CR, PR or NR on long-term outcomes. Time-independent and time-dependent Cox proportional hazards models were applied to examine the CR, PR or NR effect by adjusting for demographics, disease, and treatment characteristics.Results: O
f 277 patients, 84.5% were female. Age at LN diagnosis and lupus duration at LN were 34.32 ± 11.66 and 5.40 ± 6.47 years, respectively. Of 277 patients, 63.9% patients achieved CR, 18.41% PR, and 9.75% NR at 2 years. -CR protected from all long-term outcomes compared to PR and NR on Kaplan-Meier analysis and Cox proportional hazards model (Figure 1). However, CR protected against CV outcomes only in the Cox proportional hazards model analysis. – Compared to NR, PR only protected against low eGFR. Neither CR nor PR protected from damage accrual. On time-dependent analysis, when comparing CR to NR and PR to NR, only NR was a risk factor for ESRD when compared to CR (HR=3.93, 95% CI: 1.31-11.73, p=0.01); all the other comparisons were not statistically significant.Conclusion:
CR at 2 years from diagnosis of LN protects against CV (angina or myocardial infarction), renal (low eGFR, ESRD and composite renal outcome) outcomes and mortality. PR protects against low eGFR. Clinicians should aim for CR to prevent long-term outcomes in LN. Figure 1. Kaplan Meier analysis of long term outcome of low eGFR (<15 mL/min) among patients who achieved CR, PR or NR at 2 years of LN diagnosis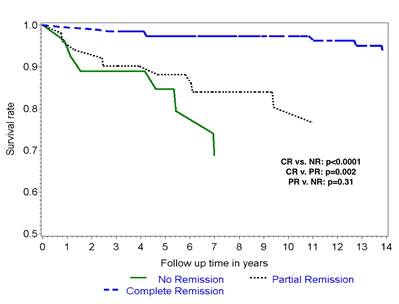
Disclosure: J. Medina-Rosas, None; D. D. Gladman, None; J. Su, None; M. Urowitz, None; Z. Touma, None.
To cite this abstract in AMA style:
Medina-Rosas J, Gladman DD, Su J, Urowitz M, Touma Z. Effect of Complete or Partial Proteinuria Recovery Compared to No Recovery at 2 Years after the Diagnosis of Lupus Nephritis on Long Term Outcomes [abstract]. Arthritis Rheumatol. 2016; 68 (suppl 10). https://acrabstracts.org/abstract/effect-of-complete-or-partial-proteinuria-recovery-compared-to-no-recovery-at-2-years-after-the-diagnosis-of-lupus-nephritis-on-long-term-outcomes/. Accessed .« Back to 2016 ACR/ARHP Annual Meeting
ACR Meeting Abstracts - https://acrabstracts.org/abstract/effect-of-complete-or-partial-proteinuria-recovery-compared-to-no-recovery-at-2-years-after-the-diagnosis-of-lupus-nephritis-on-long-term-outcomes/