Session Information
Session Type: Poster Session (Sunday)
Session Time: 9:00AM-11:00AM
Background/Purpose: IgG4-related disease (IgG4-RD) is a fibroinflammatory disorder characterized by tumefactive lesions that can occur in nearly any organ or anatomic site. Manifestations can include pancreatitis, sclerosing cholangitis, tubulointerstitial nephritis, retroperitoneal fibrosis, aortitis, and pulmonary disease. Prior to treatment and as a complication of treatment (e.g., Whipple procedure, glucocorticoids), IgG4-RD patients are at risk of organ dysfunction and failure which can lead to death. However, the risk of death in IgG4-RD is poorly understood, especially in reference to the general population. We evaluated all-cause mortality and investigated cause of death in a large cohort of IgG4-RD patients.
Methods: We identified patients seen in the Center for IgG4-RD at Massachusetts General Hospital who were diagnosed with IgG4-RD between 2010 and 2018 and had complete baseline records available for review. We determined patients’ vital statuses through the electronic medical record (EMR) and by contacting patients or next of kin. Patients were followed from the date of their first visit until date of death, last visit, or December 31st, 2018, whichever came first. Person-years (PY) of follow-up were measured and the all-cause mortality rate was calculated. We used CDC WONDER to extract expected deaths for the US general population and calculated age- and sex-standardized mortality ratios (SMR). Cause of death was determined by review of the EMR.
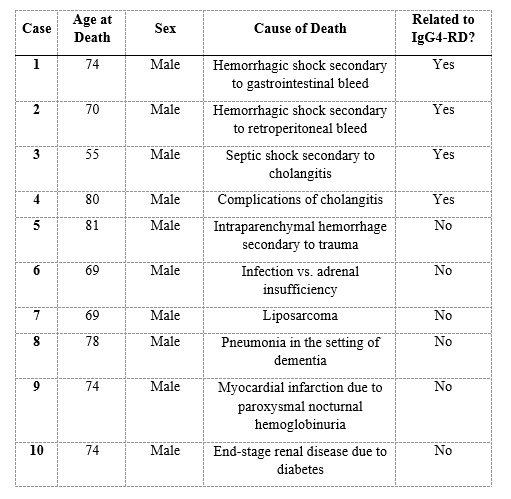
Results: We included 205 IgG4-RD patients with a mean age of 57.8 (±13.1) years; 63% were male (Table 1). During 647.7 PY of follow-up, ten patients died, yielding an all-cause mortality rate of 15.4 (95% CI 7.8-27.5) /1,000 PY. Death was associated with IgG4-RD in four (40%) cases. The first patient had pancreatic involvement and died of hemorrhagic shock secondary to a GI bleed in the setting of treatment-refractory disease. The second patient had aortic involvement and died from a retroperitoneal bleed. The third patient died of hemorrhagic shock bacteremia with gram negative bacilli in the setting of progressive cholangitis. The fourth patient died from complications related to progressive cholangitis (Table 2). Compared to the general US population, the overall SMR was 1.30 (95% CI 0.70-2.41). During follow-up, all deaths occurred in male patients. Among male patients, the all-cause mortality rate was 26.6 (95% CI: 13.5-47.4) / 1,000 PY and the corresponding SMR was 1.75 (95% CI 0.94-3.26).
Conclusion: In the early period following diagnosis, IgG4-RD mortality appears similar to that of the general population. Of the deaths related to IgG4-RD, severe pancreato-hepatobiliary disease contributed in three cases. We observed few deaths and had a relatively short follow up which may limit our power to detect significant differences in mortality. However, we observed a trend suggesting that male IgG4-RD patients may have a higher rate of death compared to the general population. Future studies with larger cohorts are necessary to further evaluate the risk of death in IgG4-RD, especially differences in late mortality. Our findings may be useful for discussing overall prognosis with IgG4-RD patients.

To cite this abstract in AMA style:
Wallwork R, Harkness T, Fu X, Perugino C, Choi H, Stone J, Wallace Z. Early Mortality in IgG4-Related Disease [abstract]. Arthritis Rheumatol. 2019; 71 (suppl 10). https://acrabstracts.org/abstract/early-mortality-in-igg4-related-disease/. Accessed .« Back to 2019 ACR/ARP Annual Meeting
ACR Meeting Abstracts - https://acrabstracts.org/abstract/early-mortality-in-igg4-related-disease/