Session Information
Title: Systemic Lupus Erythematosus - Clinical Aspects: Non-biologic Disease-modifying Antirheumatic Drugs
Session Type: Abstract Submissions (ACR)
Background/Purpose:
After achieving low disease activity or remission, immunosuppressant therapies might be stopped in lupus patients, but information on whether and how this should be done is scarce.
Our aim was to determine if tapering and withdrawing immunosuppressants in patients in remission is associated with flare.
Methods:
Analysis on all patients seen in The Lupus Clinic from 1987-2012 was conducted: 1) patients in clinical remission (no activity in the clinical SLEDAI-2K descriptors and absence of proteinuria, thrombocytopenia and leukopenia), 2) ≥ 25% taper of the immunosuppressant and 3) prednisone ≤7.5mg/day.
Flare was defined as: 1) any increase in the dosage or introduction of new immunosuppressant or 2) start or any increase of prednisone dosage.
4 groups were identified (Figure 1):
A: Flare after tapering and while still on immunosuppressant.
B: No flare but still on tapering immunosuppressant dose at last visit.
C: Flare after stopping immunosuppressant.
D: No flare after stopping immunosuppressant to last clinic visit or at 2 years.
Success was defined as no flare at last clinic visit if still on immunosuppressant (B) or no flare within 2 years following stopping the immunosuppressant (D).
Results:
Of the 1678 lupus patients registered, 204 tapering episodes in 179 patients were identified. 162 were female with age 39.0±13.3 and lupus duration 11.2±8.5 years at tapering.
Of the 204 tapering episodes 124 (61%) were successful (B and D). Immunosuppressant was stopped in 101 episodes (C and D) (table 1).
Group A and B did not reach the point of completely stopping immunosuppressant. 55 of these 103 (53.4%) flared. In group C and D 25 of 101 (24.7%) flared. In group C the time to flare was 1.7±1.0 years. In group D, all patients stopped immunosuppressant at 1.7±1.8 years and did not flare with a mean time from tapering to censoring of the data at 3.3±1.8 years (table 2).
Table 1. 204 tapering episodes
|
|
AZA |
MTX |
MMF |
P values |
|
Number of patients
|
109 |
37 |
39 |
|
|
Number of episodes N=204 |
123 |
42 |
39 |
|
|
Flare (% episodes)
|
53 (43.1%) |
17 (40.5%) |
10 (25.6%) |
X2=0.15 |
|
Completely stopped immunosuppressants (episodes) N (C+D)=101 |
58 (47.2%) |
25 (59.5%) |
18 (46.2%) |
X2=0.34 |
Figure 1. Grouping of patients
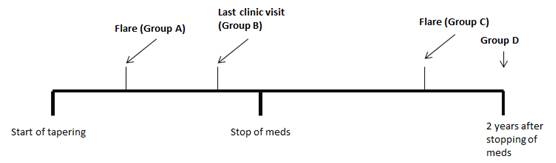
Table 2. Mean time to event results (years)
|
Group |
Time to stop event |
Time to stop immunosuppressant |
Time stop immunosuppressant to event |
|
A n=55 |
1.5±1.2 |
N/A |
N/A |
|
B n=48 |
2.1±2.5 |
N/A |
N/A |
|
C n=25 |
1.7±1.0 |
0.9±0.9 |
0.8±0.5 |
|
D n=76 |
3.3±1.8 |
1.7±1.8 |
1.6±0.6 |
Conclusion:
Our results suggest that successful tapering and discontinuation of immunosuppressants is possible in about 1/2 of clinically stable patients. In 1/4 a subsequent flare occurred. Future research may identify which patients are most likely to successfully discontinue immunosuppressants and define an appropriate algorithm for immunosuppressant tapering.
Disclosure:
Z. Touma,
None;
M. B. Urowitz,
None;
D. Ibanez,
None;
D. D. Gladman,
None.
« Back to 2013 ACR/ARHP Annual Meeting
ACR Meeting Abstracts - https://acrabstracts.org/abstract/do-we-know-how-and-when-to-taper-and-stop-in-immunosuppressants-in-lupus-patients/