Session Information
Session Type: Abstract Submissions (ACR)
Background/Purpose: Inflammation plays a key role in the progression and destabilisation of atherosclerotic plaque in the general population. In RA, inflammation is thought to accelerate atherosclerosis and may lead to a more unstable plaque phenotype. 18F-Fludeoxyglucose PET-CT (FDG-PET-CT) is a nuclear imaging technique which can be used to quantify carotid plaque inflammation. Histology studies have shown that FDG-uptake correlates with macrophage content of plaque and it has been used to identify vulnerable lesions and evaluate the effects of statins. We hypothesised that patients with active arthritis would have carotid plaque inflammation on FDG-PET and that plaque inflammation would correlate with the degree of disease activity using the DAS-28 score.
Methods: Patients with active arthritis (DAS-28>3.2), who had evidence of carotid plaque on ultrasound, were invited to have MRI then an FDG-PET-CT scan of the carotid arteries. Those on statins, or those with a history of cancer or recent infection, were excluded.
Following MRI scans performed on a 3 Tesla scanner, patients subsequently attended for a PET-CT within 2 weeks. FDG tracer was injected after a 6 hour fast. The scan was performed 2 hours after injection. Patients were positioned in a specialist head support to mimic MRI position. Mandible to sternal notch distance was also measured to ensure similar positioning during the 2 scans.
T1-weighted sequences from the MRI and PET-CT images were co-registered, then a region of interest (ROI) was drawn round the plaque. FDG uptake in the ROI was measured by a physicist, blinded to clinical information. The tissue activity was divided by the injected activity per kilo to give a maximum standardised uptake value (SUVmax). Descriptive and non-parametric statistical analyses were performed.
Results: 12 patients underwent MRI and FDG-PET-CT, 8 of whom were female. The median (IQR) age and disease duration was 59.5 (56.5, 64.5) and 11 (5.5, 25) years, respectively. The median DAS-28 score was 4.52 (4.32, 5.13) and 10 patients were rheumatoid factor and/or ACPA positive. No patients had a history of arterial disease, 2 had hypertension, 1 had dyslipidaemia and 2 were smokers.
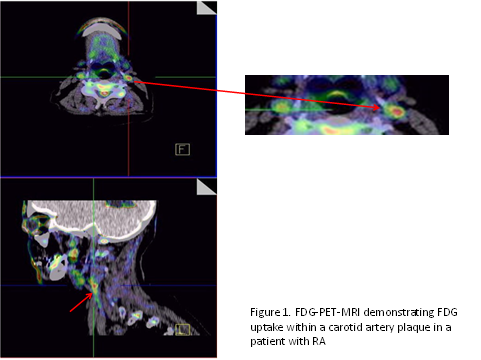
The median plaque thickness was 2.5 (2.3, 2.8) mm and all had less than 70% stenosis. All subjects had plaque inflammation on PET-MRI, median (range) SUVmax was 2.14 (1.46, 6.11). An example of a PET-MRI can be seen in figure 1. There was no significant correlation with SUVmax and DAS28 or erythrocyte sedimentation rate (r=0.126, p=0.70 and r=-0.15, p=0.63 respectively).
Conclusion: Plaque inflammation was demonstrated in all subjects, despite the cohort having no history of cardiovascular disease and relatively small lesions. Larger longitudinal studies are required to further investigate the relationship between disease activity and plaque inflammation and to study the effects of inflammation on plaque progression.
Disclosure:
S. Skeoch,
None;
H. Williams,
None;
P. Cristanacce,
None;
J. James,
None;
P. Hockings,
None;
Y. Alexander,
None;
J. Waterton,
None;
I. N. Bruce,
None.
« Back to 2014 ACR/ARHP Annual Meeting
ACR Meeting Abstracts - https://acrabstracts.org/abstract/do-patients-with-active-ra-also-have-inflamed-atherosclerotic-plaques-on-pet-mri/