Session Information
Date: Saturday, November 16, 2024
Title: Vasculitis – Non-ANCA-Associated & Related Disorders Poster I
Session Type: Poster Session A
Session Time: 10:30AM-12:30PM
Background/Purpose: Biologic DMARDs (bDMARDs) are mainstay in management of patients with difficult to treat Takayasu Arteritis (D2TTAK). The cost of long-term biologics is prohibitory in resource poor countries. The transcriptome studies suggest involvement of IL-1 signalling and JAK-STAT pathways in pathogenesis in TAK. Colchicine (Col) is an anti-mitotic, anti-inflammatory agent which acts on neutrophils, macrophages and IL-1 pathway and exerts antifibrotic effect on arterial wall in patients with cardiovascular disease.
In this study we report the efficacy of colchicine, as compared with tofacitinib (Tofa) in patients with D2TTAK.
Methods: Clinical, laboratory and imaging details of patients satisfying ACR EULAR 2022 criteria for TAK who received Tofa or Col across 5 centres in India were recorded retrospectively. D2TTAK defined as patients who are unable to achieve remission with conventional synthetic DMARDs (csDMARD) were included. The disease was considered active based on a composite criterion which required presence of any two of the three parameters a) new clinical symptoms as evidenced by Indian Takayasu arteritis score ITAS >1 b) persistently raised CRP for 2 consecutive visits c) new areas of arterial wall thickening/stenosis/aneurysm in angiography or active uptake in 18FDG PETCT imaging.
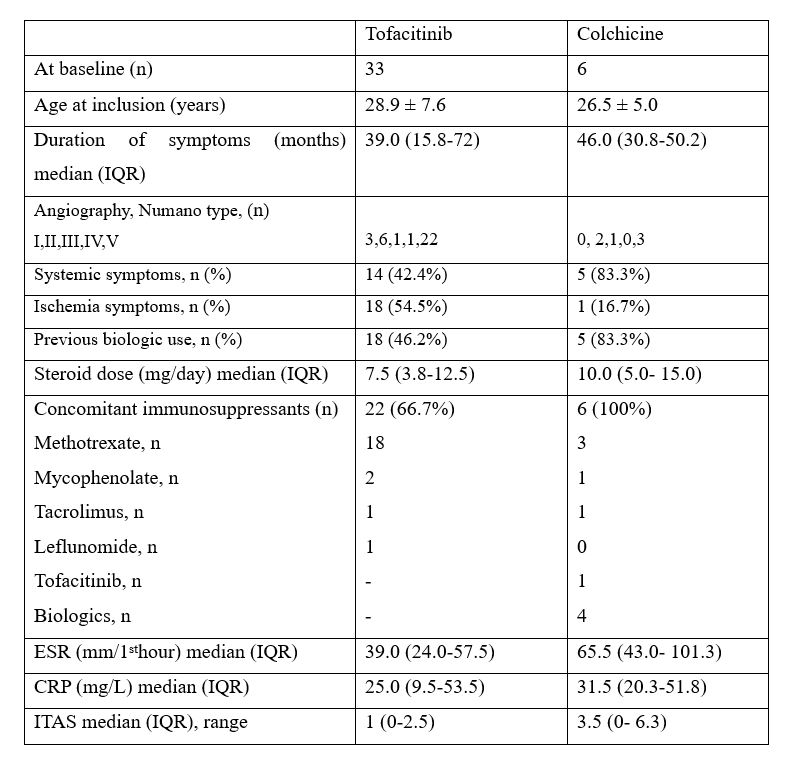
Results: Among, 41 patients initiated on Tofa or Col, 39 patients were D2TTAK (Tofa-33 and Colchicine-6) and hence were included. Colchicine was given as an add on therapy to the existing DMARDs for all patients. The baseline characteristics are presented in table-1.
The patients who were initiated on tofacitinib received a median of 2 (1-3.5) lines of prior DMARDs. The indication for initiating Tofa was clinically active disease and persistent laboratory activity in 24 (72.7%) and 20 (60.6%) patients respectively while 7 (21.2%) had activity on imaging in-spite of non-biologics or biologic DMARDs.
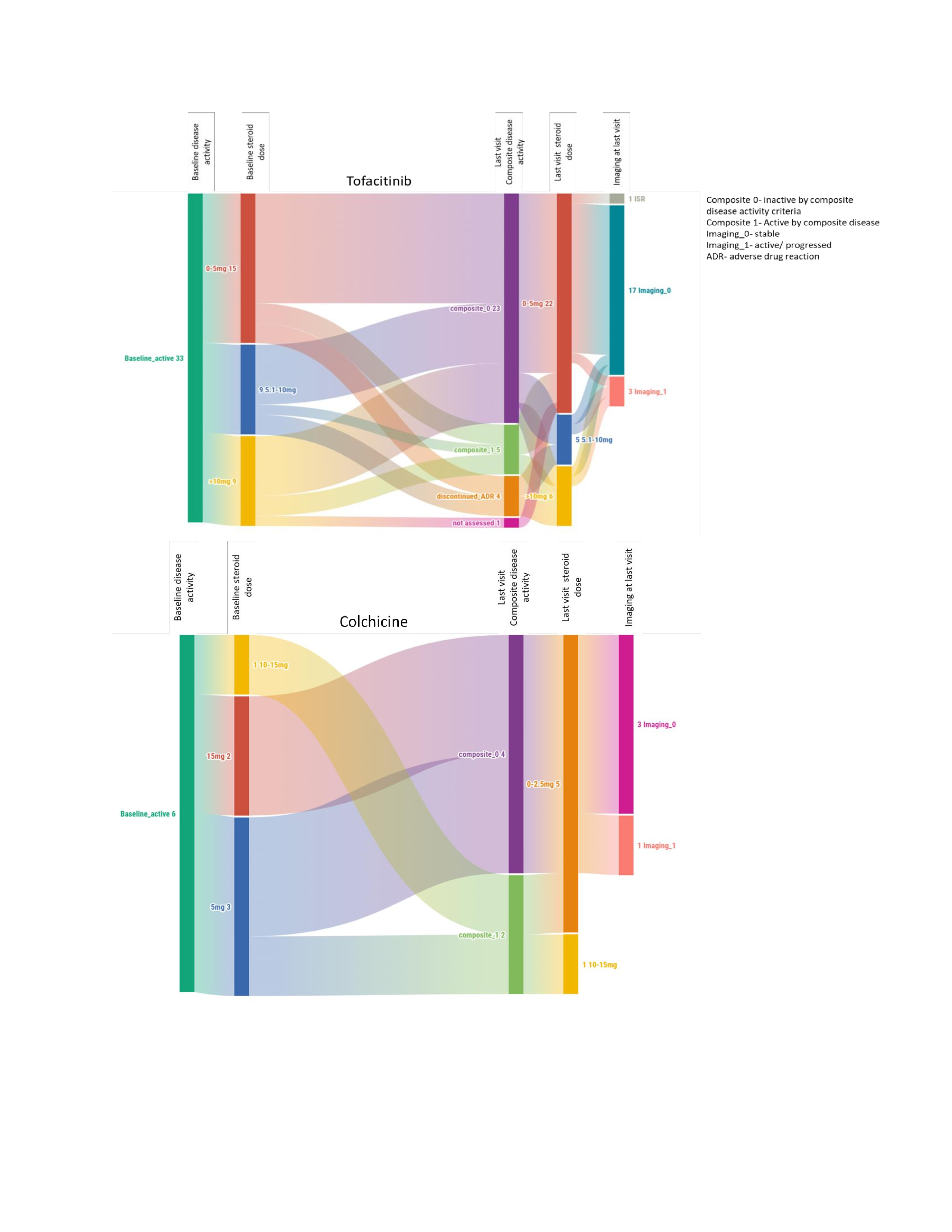
During a follow-up of 15.0 (6.5-20.0) months, 23 (69.7%) of patients on Tofa satisfied the composite criteria for inactive disease (Figure-1A). Among patients with bDMARD-NR (n-18), 14 (77.8%) achieved inactive disease. Nine patients discontinued Tofa due to lack of induction of response in 5 (15.2%) and adverse events in 4. One patient had an increase in ITAS score which was attributed to the in-stent restenosis of previously revascularized vessel was excluded from analysis due to difficulty in disease assessment.
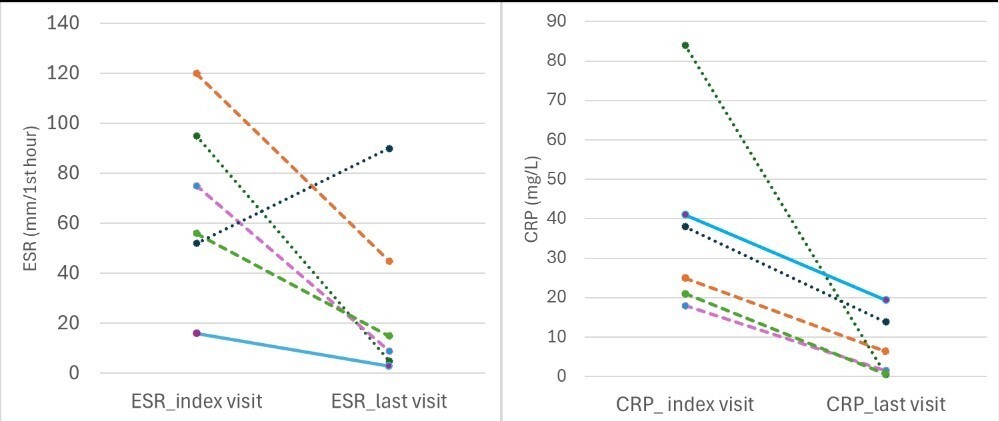
The patients on Colchicine received median of 4 (3-6) lines of prior DMARDs. The indications were clinically active disease with persistently high CRP or imaging activity in 4 patients and persistently high CRP in 2 patients. During a follow up of 7.5 (6-9.3) months, 4 patients (66.7%) in Col group attained inactive disease as per composite outcome (Figure-1B). Another 1 patient achieved stable disease but relapsed after withdrawing the baseline tacrolimus while one patient had active disease at the last visit. The CRP and ESR decreased after initiation of Col (Figure-2). No adverse event was observed.
Conclusion: In this first ever report of use of add-on colchicine in D2TTAK, efficacy of colchicine was comparable to Tofacitinib for inducing inactive disease.
To cite this abstract in AMA style:
Kumar R, Vasanth P, Janardhana R, Ganapati A, Patil A, Jain A, Pinto B, Jois R, Padiyar S, Mathew J, Shobha V, Joseph G, goel R. Difficult to Treat Takayasu Arteritis: Comparative Efficacy of Colchicine and Tofacitinib [abstract]. Arthritis Rheumatol. 2024; 76 (suppl 9). https://acrabstracts.org/abstract/difficult-to-treat-takayasu-arteritis-comparative-efficacy-of-colchicine-and-tofacitinib/. Accessed .« Back to ACR Convergence 2024
ACR Meeting Abstracts - https://acrabstracts.org/abstract/difficult-to-treat-takayasu-arteritis-comparative-efficacy-of-colchicine-and-tofacitinib/