Session Information
Session Type: Abstract Submissions (ACR)
Background/Purpose: Several biologics therapy reportedly regress gastric amyloid deposition in amyloid A (AA) amyloidosis patients with rheumatoid arthritis (RA), but it is uncertain whether the biologics therapy can also reduce renal amyloid deposition or not, because it is difficult to repeat a renal biopsy in these patients. We classified renal amyloidosis into two groups, glomerular and vascular types (J. Rheumatology, 2006, 1). In patients with vascular type disease, renal involvements are limited, which enabled us to carry out a follow-up histological study. The main focus of the present study is to compare the regression of amyloid deposition in kidney before and after biologics treatment in patients with vascular type disease.
Methods: The diagnosis of AA amyloidosis was determined by Congo-red stain and anti-AA antibody of gastric biopsy specimen. At first, the RA patients with AA amyloidosis were treated with methotrexate and 5mg of prednisolone, but they did not achieve adequate responses. Subsequently, they were treated with tocilizumab or etanercept for more than three years. Gastric and renal biopsies were performed before and after biologics treatment at least three years’ interval. Renal biopsies were examined only in patients with AA amyloidosis of vascular type disease because renal function does not significantly deteriorate (1).
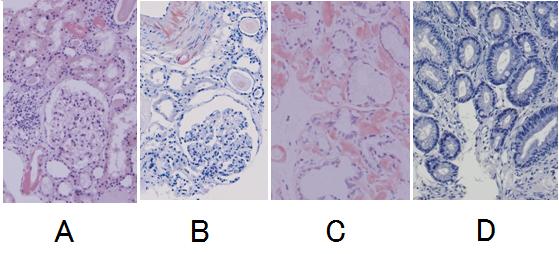
Results: The vascular type of AA amyloid patients with RA received either etanercept or tocilizumab and the clinical symptoms and laboratory data were significantly improved and sustained for more than 3 years during treating with the biologics. Before biologics treatment, renal biopsy specimens showed amyloid deposition around the blood vessels selectively (Figure A). After biologics treatment (mean 4.5 years), however, amyloid deposition did not significantly regress, similar to those observed in the initial study (Figure B). Renal function of the patients was not also changed significantly. The results of AA deposition in kidney were also confirmed by anti-AA antibody. In the gastrointestinal tract, after treatment (mean 4.5 years) with etanercept or tocilizumab, amyloid deposition was markedly regressed (Figure D) compared to the initial study (Figure C) as reported.
Conclusion: Amyloid deposition of the kidney, unlikely to the gastric tract, does not significantly regress in AA amyloidosis patients with RA by biologics therapy, suggesting that regression of amyloid deposition is differently regulated between the kidney and the gastric tract.
References: 1. Two distinct clinical courses of renal involvement in rheumatoid patients with AA amyloidosis. J Rheumatol. 2006;33:1482-7.
Figure
Results of renal biopsy (A, B) and gastrointestinal biopsy (C, D) before therapy (A, C) and after therapy (B, D) by etanercept. (Congo red stained; original magnification x 200.)
Disclosure:
H. Uda,
None;
T. Harada,
None;
A. Matsumoto,
None;
A. Mizumoto,
None;
T. Takama,
None;
O. Saiki,
None.
« Back to 2013 ACR/ARHP Annual Meeting
ACR Meeting Abstracts - https://acrabstracts.org/abstract/differential-effects-of-biologics-on-the-removal-of-amyloid-deposition-between-the-kidney-and-gastric-tract-of-amyloid-a-amyloidosis-patients-with-rheumatoid-arthritis/