Session Information
Date: Monday, November 9, 2015
Title: Miscellaneous Rheumatic and Inflammatory Diseases Poster Session II
Session Type: ACR Poster Session B
Session Time: 9:00AM-11:00AM
Background/Purpose: Sarcoidosis is
a multisystemic disorder of unknown
cause. About 30-60% of
patients have ocular involvement
consistent in bilateral uveitis. Recently, the
clasification criteria proposed by
the First International
Workshop on Ocular Sarcoidosis (FIWOS) has been validated.
The criteria classifies ocular sarcoidosis
as definite (uveitis and biopsy
positive), presumed
(bilateral hilar lymphadenophaty and uveitis without
biopsy), probable (3 ocular signs and
2 laboratory tests without biopsy
and without bilateral hilar lymphadenopathy)
and possible (4 ocular
signs and 2 laboratory tests
with negative biopsy) based of
specific ophthalmological and laboratory findings.
This classification is useful especially
when a biopsy is
not avalilable or when it
is negative./Categorization of patients diagnosed
with ocular sarcoidosis
according to the criteria
proposed by the FIWOS in the
last five years in a uveitis unit
of the University Hospital Donostia in Guipœzcoa,
Spain.
Methods: The clinical records
of patients diagnosed
with ocular sarcoidosis
were reviewed retrospectively.
The variables measured were age, sex,
systemic manifestations, pattern of uveitis,
Quantiferon test, angiotensin converting
enzyme, biopsy, chest
radiography and treatment. The patients then
were classified based
on the criteria of
the FIWOS.
Results: A total of 11 patients
were diagnosed with
sarcoid uveitis, 7 females
(63.6%) and 4 males (36.3%). The median age was 58.0 years (SD 20.5). In 7 patients (63.3%) uveitis was the
first manifestation of
the disease, 5 of
them later developed
systemic symptoms and 2 showed
isolated eye involvement. The remaining 4 patients
(36.3%) showed systemic symptoms of:
bilateral hilar adenopathy in 81.8%, respiratory symptoms 36.3%, peripheral adenopathy
18.1%, parotitis in 27.2% and erythema nodosum
in 9.0%. The patterns of uveitis most
frequently observed were bilateral panuveitis in 54.5%, chronic unilateral anterior uveitis
in 27.2% and chronic bilateral anterior uveitis in 18.1%. The categorization of patients
revealed a diagnosis of definite sarcoidosis
in 4 (36.3%), presumed in 5
(45.4%), probable in 1 (9.0%) and
possible in 1 patient (9.0%). The most common treatment was methotrexate in 45.4%. Two
patients were treated withanti-TNF
Conclusion: 81.7% of our patients were
categorized as having definite or presumed
sarcoidosis. More than half of our
patients who had no
confirmatory biopsy were diagnosed
of ocular sarcoidosis.
Bilateral panuveitis and chronic anterior uveitis were the most frequent ocular patterns.
Most patients with ocular involvement
developed subsequently systemic symptoms.
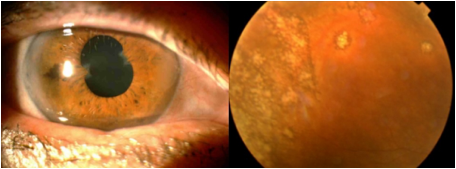
A. B
A. Peripheral anterior synechiae after complicated uveitis.
B.
Multiple chorioretinal lesions.
To cite this abstract in AMA style:
Meneses Villalba CF, Maiz Alonso O, Blanco A, Egües Dubuc CA, Uriarte Ecenarro M, Errazquin Aguirre N, Valero JA, Belzunegui Otano JM. Diagnostic Categorization of Ocular Sarcoidosis Based on the International Criteria Proposed By the First International Workshop on Ocular Sarcoidosis. a Case Series of 11 Spanish Patients [abstract]. Arthritis Rheumatol. 2015; 67 (suppl 10). https://acrabstracts.org/abstract/diagnostic-categorization-of-ocular-sarcoidosis-based-on-the-international-criteria-proposed-by-the-first-international-workshop-on-ocular-sarcoidosis-a-case-series-of-11-spanish-patients/. Accessed .« Back to 2015 ACR/ARHP Annual Meeting
ACR Meeting Abstracts - https://acrabstracts.org/abstract/diagnostic-categorization-of-ocular-sarcoidosis-based-on-the-international-criteria-proposed-by-the-first-international-workshop-on-ocular-sarcoidosis-a-case-series-of-11-spanish-patients/