Session Information
Session Type: ACR Poster Session A
Session Time: 9:00AM-11:00AM
Background/Purpose: Patients with rheumatoid arthritis (RA) and systemic lupus erythematosus (SLE) have an increased risk of premature cardiovascular disease (CVD), making comorbid risk factors like smoking a prime intervention target for rheumatology patients who smoke. Primary care clinics have systems to promote cessation, but rheumatology clinics rarely address smoking adequately (Vreede 2015). Resources like free telephone quit lines exist that have already been shown to improve the odds of quitting, but patients must first be connected to them. The Ask-Advise-Connect model has been shown to increase the proportion of patients being referred to quit lines 13-fold (Vidrine 2013), but this model has not been studied thoroughly in specialty clinics. These tools show great promise for encouraging tobacco cessation, but they should be tailored for use in rheumatology in order to maximize their effectiveness. Our goal was to work with rheumatology clinic staff to 1) understand current tobacco cessation care practices and obstacles and 2) use that information to customize and implement a quit line referral intervention based on the Ask-Advise-Connect model.
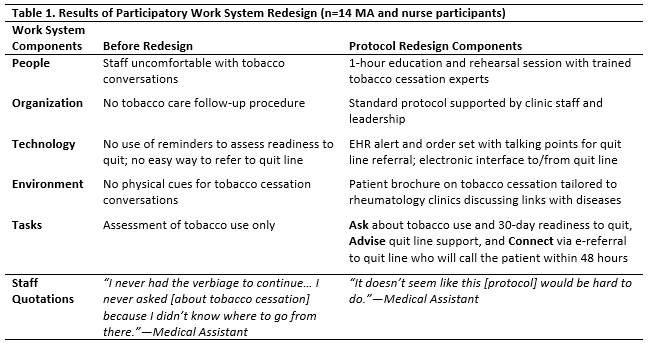
Methods: We conducted participatory work system redesign with medical assistants (MAs) and nurses from three rheumatology clinics at a large, academic health system in 2015. Building on prior patient and provider interviews and staff focus groups, we held two hour-long focus groups using semi-structured interview questions to assess current processes, needs, and a proposed electronic health record (EHR)-based quit line referral process. The results were organized according to the Systems Engineering Initiative for Patient Safety (SEIPS) work system domains.
Results: 80% (9 MAs, 5 nurses) of the clinic staff participated in the focus groups. We found that smoking assessment was standard, but follow-up actions were rare. Barriers to assessing smoking and referring patients to cessation resources included discomfort discussing cessation with smokers and the absence of an easy referral process (Table 1). Using these findings, we developed a new staff-driven tobacco quit line referral process for MAs and nurses that leverages our EHR system. The process uses two decision-support EHR alerts with conversation prompts to assess use and 30-day readiness to quit (Ask), encourage cessation (Advise), and refer the patient to the state tobacco quit line using an electronic interface (Connect). We also created a rheumatology-specific educational brochure and an hour-long staff training program to support the workflow.
Conclusion: By working directly with our rheumatology MAs and nurses, we developed a new smoking assessment and referral protocol that addresses major obstacles to delivering consistent, effective care to rheumatology patients who smoke. We are testing the effectiveness of this intervention in a 6-month pilot.
To cite this abstract in AMA style:
Panyard D, Ramly E, Gilmore-Bykovskyi A, Lauver D, Adsit R, Maxcy C, Bartels CM. Developing a Staff-Driven Electronic Smoking Cessation Referral Program in Rheumatology Clinics [abstract]. Arthritis Rheumatol. 2016; 68 (suppl 10). https://acrabstracts.org/abstract/developing-a-staff-driven-electronic-smoking-cessation-referral-program-in-rheumatology-clinics/. Accessed .« Back to 2016 ACR/ARHP Annual Meeting
ACR Meeting Abstracts - https://acrabstracts.org/abstract/developing-a-staff-driven-electronic-smoking-cessation-referral-program-in-rheumatology-clinics/