Session Information
Session Time: 6:00PM-7:00PM
Background/Purpose: Chronic anterior uveitis (CAU) occurs in 10-20% of JIA patients, yet the factors driving risk for JIA-associated uveitis (JIA-U) are not established. The HLA alleles associated with JIA and CAU are different. Here we identify clinical characteristics and HLA Class I and Class II four digit alleles associated with JIA-U.
Methods: In this prospective study – Predicting Eye Disease In childhood Arthritis-Uveitis (PEDiA-U), we enrolled patients with JIA-U and those with JIA without uveitis (JIA-no-U) who had a disease duration of >4 years. This definition of JIA-no-U based on ~85% of JIA-U patients develop CAU within 4 years of JIA diagnosis. Genotyping was done on the Illumina Infinium Omni2.5 beadchip (2.3 million markers). HiBag was used for HLA ClassI/II imputation with population structure estimated using Admixture; five admixture estimates were included as covariates in logistic regression models that tested for association between each four-digit allele and JIA-U/JIA-no-U. The models accounted for imputation uncertainty via modeling allele dosage.
Results: Demographics of the 215 JIA-U cases/ 430 JIA-no-U cases are compared in Table 1. Compared to JIA-no-U, JIA-U were significantly younger at JIA onset (mean±SD 4.1±3.3 years vs 6.7±4.6, respectively, P=0.0012). The most common JIA subtypes were oligoarticular and polyarticular RF-negative JIA, with significant differences in JIA-U rates among subtypes (P=2.92 x10-6). JIA-U were more often ANA positive (P=3.55 x10-7). Treatment strategies differed between JIA-U and JIA-no-U within first year (P=0.0005). Time to initiate MTX treatment was earlier in patients with JIA-no-U (P=0.008) (Table 1).
Five HLA Class I and II four-digit alleles were associated with JIA-U (Table 2; P< 1x10-6), including DQA1*05:05 (odds ratio OR=1.90), DQA1*01:01 (OR=0.40), DRB1*01:01 (OR=0.39), DRB1*11:04 (OR=2.94) and DRB1*11:01 (OR=2.64). Although well-established JIA-associated alleles like DRB1*08:01 were identified, they were less significant (OR=1.74, P=0.0002) as was idiopathic CAU risk loci HLA-DQB1*04:02 (OR=1.58, P=0.0006). HLA-B27 alleles were not statistically significant.
Conclusion: The HLA risk profile for JIA-U differs from that of JIA-no-U and HLA-B27-associated uveitis. We corroborate four-digit allele associations for JIA-U for DRB1*11:04 and DRB1*11:01. ANA positivity, JIA subtype, and young age at JIA onset were also validated as clinical risk factors. Ongoing work includes JIA-U GWAS to identify associated loci outside the HLA region, linking loci to genes and biologic pathways for potential therapeutic targets, and the development of a polygenic risk score.
Clinical characteristics of patients with JIA and JIA-associated uveitis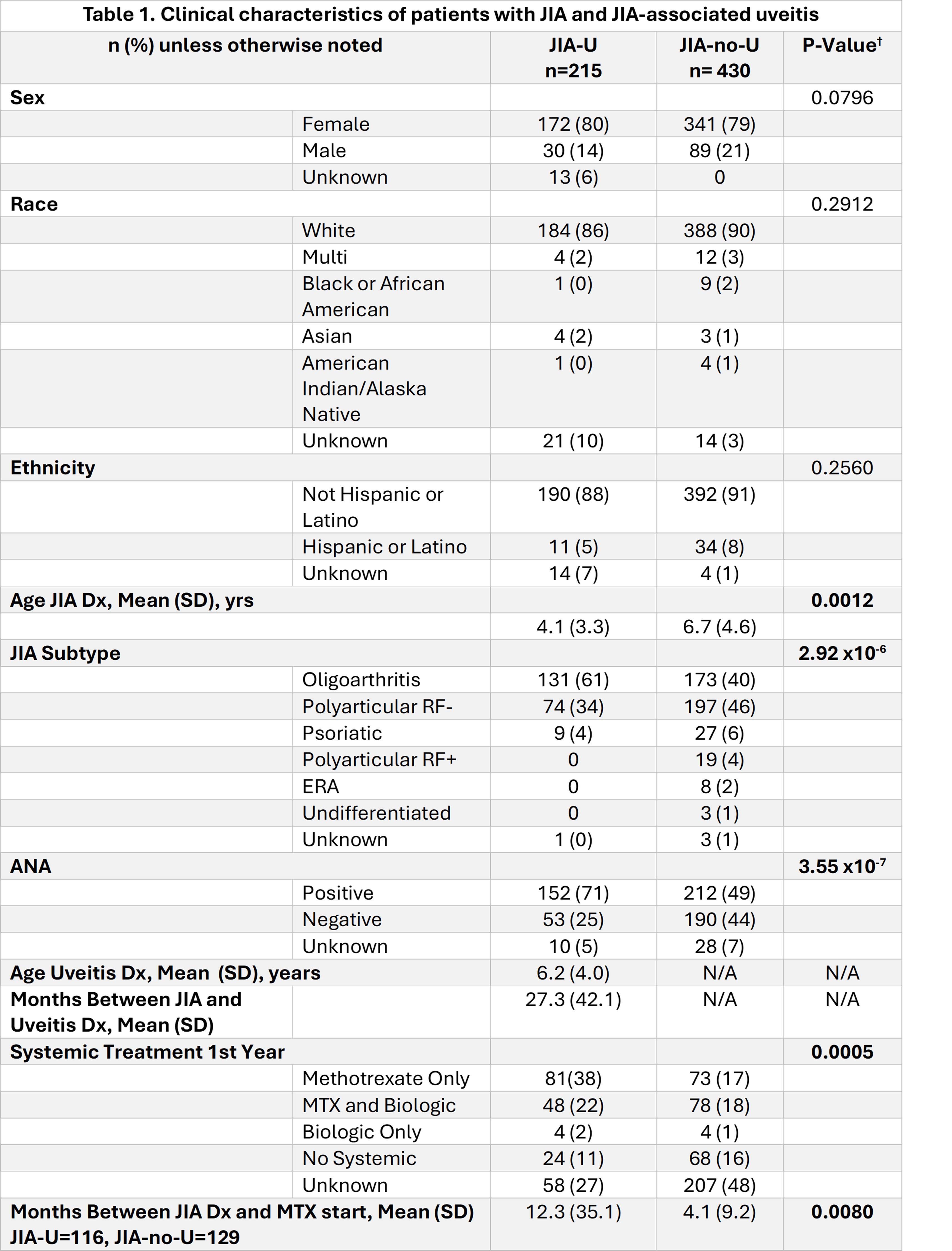
Top 15 HLA Class I and II alleles associated with JIA-associated Uveitis from PEDiA-U Cohort.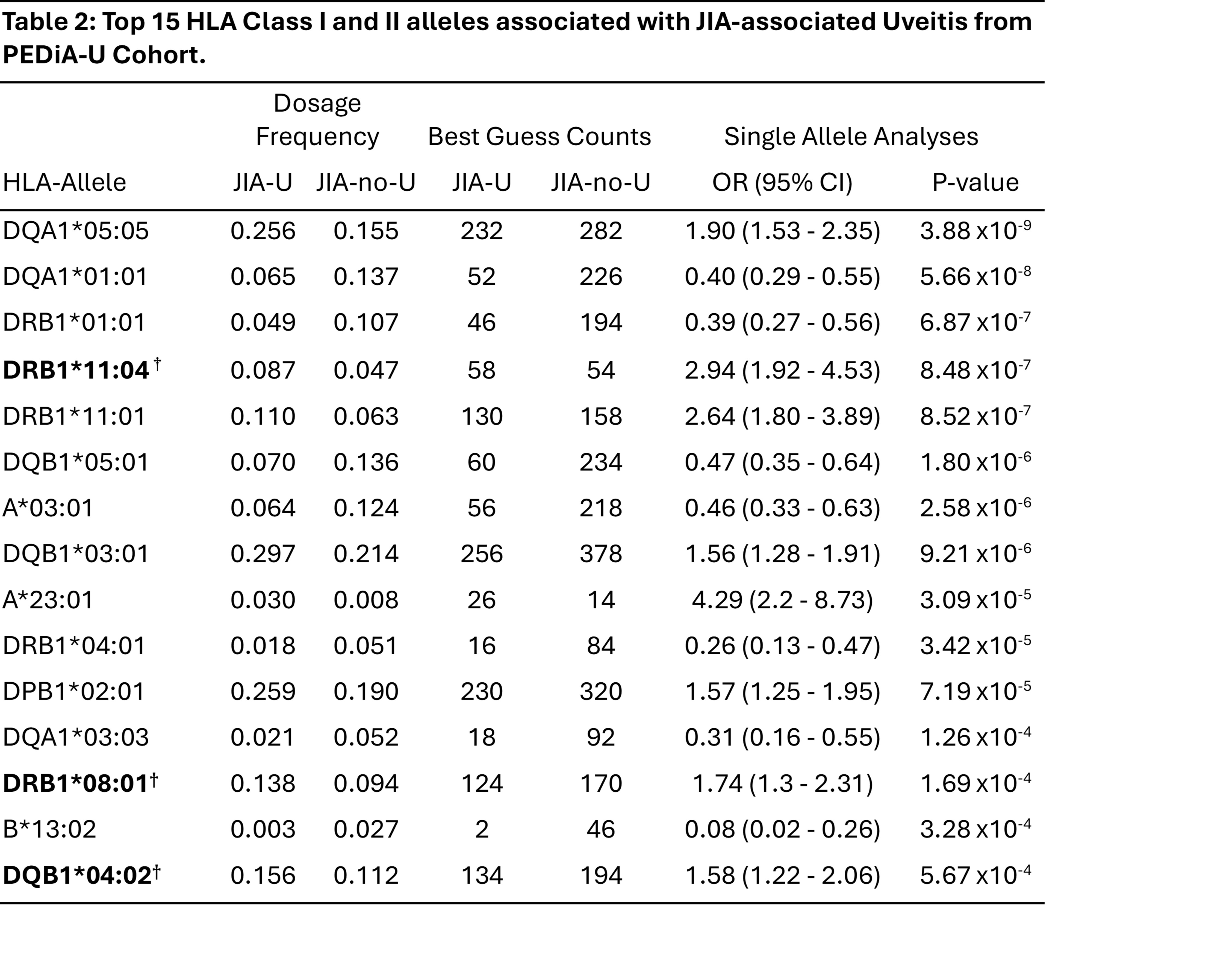
To cite this abstract in AMA style:
Angeles-Han S, Thompson S, Brunner H, Ainsworth H, Altaye M, Aundhia M, Bohnsack J, Chang M, cooper a, Davidson S, Duell A, Howard T, Lerman M, Lo M, Maccora I, Marion M, Nihalani-Gangwani B, Prahalad S, Reina C, Quinlan-Waters M, Schulert G, Simonini G, Speer C, stahl e, Sudman m, Miraldi Utz V, Wagner M, Langefeld C. Demographic, Clinical and Major Histocompatibility Complex (MHC) variation associated with uveitis development in children with juvenile idiopathic arthritis [abstract]. Arthritis Rheumatol. 2026; 78 (suppl 3). https://acrabstracts.org/abstract/demographic-clinical-and-major-histocompatibility-complex-mhc-variation-associated-with-uveitis-development-in-children-with-juvenile-idiopathic-arthritis/. Accessed .« Back to 2026 Pediatric Rheumatology Symposium
ACR Meeting Abstracts - https://acrabstracts.org/abstract/demographic-clinical-and-major-histocompatibility-complex-mhc-variation-associated-with-uveitis-development-in-children-with-juvenile-idiopathic-arthritis/