Session Information
Date: Tuesday, November 15, 2016
Title: Spondylarthropathies and Psoriatic Arthritis – Clinical Aspects and Treatment - Poster III
Session Type: ACR Poster Session C
Session Time: 9:00AM-11:00AM
Background/Purpose: Disease Activity index for Psoriatic Arthritis (DAPSA) originally developed from patients with reactive arthritis and validated in psoriatic arthritis (PsA) patients. DAPSA includes swollen joint count (SJC) (66 joint), tender joint count (TJC) (68 joint), CRP (mg/dl), patient global assessment and pain. Although, assessment of 66/68 joints give more information, 28 joint assessment is more feasible, and frequently used in rheumatoid arthritis trials. Objective of this study was to assess correlation of DAPSA 28 joints with DAPSA 66/68 joints in a multicenter PsA registry.
Methods: PsART (Psoriatic Arthritis Registry of Turkey) is a national, web-based registry, including 1081 PsA patients. Overall, 601 patients had complete information about DAPSA score. All affected joints were recorded separately. Original DAPSA calculated to sum of CRP (mg/dl), pain VAS (cm), patient’s global assessment of disease activity VAS (cm), SJC (66 joints), and TJC (68 joints). We calculated both 28 TJC/SJC (called DAPSA-28) and 66/68 joints for DAPSA. Spearman correlation was used for statistical analysis.
Results: 396 of 601 (65.9%) were female, mean age was 46.5 (12.6) years, mean PsA duration was 5.4 (6.6) years. Mean DAPSA 66/68 score was 14.5 (13.3) and DAPSA 28 score was 12.9 (9.7). Correlation of DAPSA 66/68 and DAPSA 28 was 0.97. Correlation of SJC 28 and SJC 66 was 0.83 and correlation of TJC 28 and TJC 68 was 0.88. Correlation of TJC 28 and 68 were shown in figure 1. 374 of 601 (62.2%) patients at least one active joint according to 66/68 joint assessment. When we consider those group, correlation coefficients were slightly unfavorable in TJC and SJC (SJC 28 vs 66 r=0.78, TJC 28 vs TJC 68 r=0.78), however almost identical in their DAPSA scores (DAPSA 28 vs DAPSA 66/68 r=0.94). Patients with swollen MTF, ankle and DIF joints were 41 (6.8%), 67 (11.1%), and 60 (10.0%), respectively. By doing a 28 joint count, 47 (7.8%) were missed compared to 66/68 joint count due to the DIP, MTF and ankles being the only site of arthritis.
Conclusion: DAPSA domains are almost universal for all kind of inflammatory arthritis. Simple sum of those domains seem valid and feasible in PsA patients. Although assessment of 66/68 joints is rationalized particularly for patients with distal interphalangeal and foot arthritis, our study showed that there was no added value of using 66/68 joints in the real life setting. On the other hand, almost 8% of patients did not capture when assess only 28 joints. 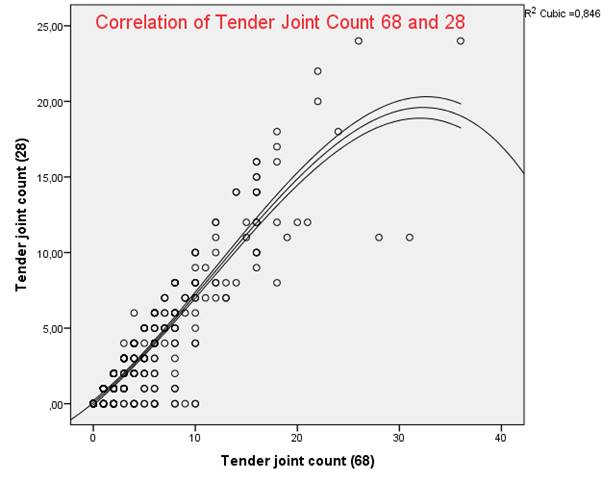
To cite this abstract in AMA style:
Kalyoncu U, Bayndır O, Oksuz MF, Kimyon G, Erden A, Yavuz S, Cetin G, Kucuksahin O, Kilic L, Omma A, Ozisler C, Solmaz D, Onat AM, Kisacik B, Ersozlu Bakirli D, Cinar M, Tufan A, Yildiz F, Mercan R, Kasifoglu T, Yilmazer B, Yilmaz S, Aksu K, Erten S, Sayarlioglu M, Dalkilic E, Akar S, Acikel C, Aydin Tufan M, Balkarli A, Kasapoglu-Gunal E, Senel S, Kobak S, Duruoz MT, Dogru A, Tarhan EF, Can M, Akyol L, Pehlevan S, Erbasan F, Arslan F, Kucuk A, Gonullu E, Kabasakal Y, Sahin M, Atakan N, Aydin SZ. Dapsa-28 May be Used Instead of Dapsa-66/68 in Psoriatic Arthritis [abstract]. Arthritis Rheumatol. 2016; 68 (suppl 10). https://acrabstracts.org/abstract/dapsa-28-may-be-used-instead-of-dapsa-6668-in-psoriatic-arthritis/. Accessed .« Back to 2016 ACR/ARHP Annual Meeting
ACR Meeting Abstracts - https://acrabstracts.org/abstract/dapsa-28-may-be-used-instead-of-dapsa-6668-in-psoriatic-arthritis/