Session Information
The 2020 Pediatric Rheumatology Symposium, originally scheduled for April 29 – May 2, was postponed due to COVID-19; therefore, abstracts were not presented as scheduled.
Date: Saturday, May 2, 2020
Title: Poster Session 3
Session Type: ACR Abstract Session
Session Time: 4:15PM-5:15PM
Background/Purpose: Intravenous immunoglobulin (IVIG) effectively treats vasculitis of the coronary arteries in the large majority of Kawasaki Disease (KD) patients. However, approximately 25% of patients develop coronary artery aneurysms (CAA) in the first 12 weeks of illness and 1% will advance to giant CAA. Herein, we describe our experience with the use of cyclophosphamide (CYC) for the treatment of giant or rapidly progressing CAA in children with KD.
Methods: We performed a retrospective chart review of KD patients treated with CYC from 01/2006-12/2019 at Boston Children’s Hospital. Clinical and echocardiographic data were summarized.
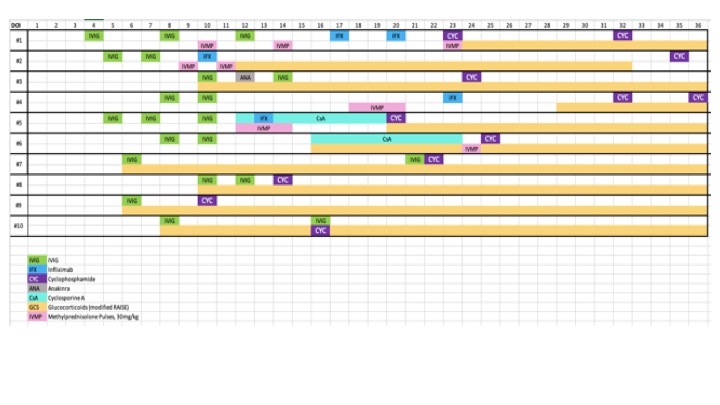
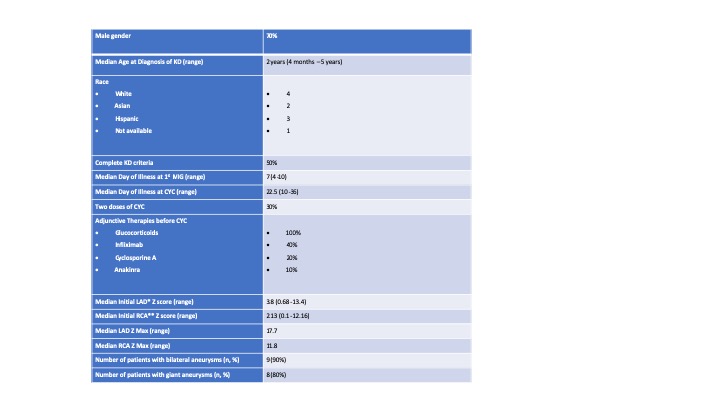
Results: Ten patients (7 male, 3 female), median age 2.0 years (range 4 months -5 years), representing 5% of all patients with CAA during the study period were treated with CYC (10 mg/kg intravenously for 1 or 2 doses). (Table 1). All patients were initially treated with IVIG between Day 4-10 of fever onset. Other anti-inflammatory treatments administered before CYC included second IVIG dose (8), corticosteroids (n=8), infliximab (n=4), cyclosporine (n=2), and anakinra (n=1). Median illness day at first CYC dose was 22.5 days (10-36 days). (Figure 1). The primary indication for treatment for all 10 patients was IVIG resistance and/or rapid progression of coronary artery aneurysms. Three patients received a second dose of CYC (10mg/kg) one week following the first dose for progressively enlarging CAA . No further immunosuppressive treatment was given after the last CYC other than oral steroids. Coronary artery maximum z scores (zMax) were above 10 in eight of ten patients with a median zMax 15.65 (IQR 8.96-25.03) of the left anterior descending artery and 11.75 (IQR 7.4-14.2) of the right coronary artery. CAA did not progress after CYC treatment. (Figure 2). One patient with a history of neutropenia in infancy developed severe neutropenia (absolute neutrophil count (ANC) of 100 /ml3) 9 days after treatment with CYC. He recovered without intervention with a normal ANC at 3 months follow up. No patients developed infections or other serious toxicity from CYC.
Conclusion: In a small series of KD patients with progressive enlargement of coronary artery aneurysms despite aggressive anti-inflammatory therapy, CYC seemed to arrest further dilation and was well-tolerated. This is the largest case series reporting the use of CYC in the literature, and the first to propose standardized course of treatment. CYC may be considered for treating children with severe, refractory KD resistant to other agents.
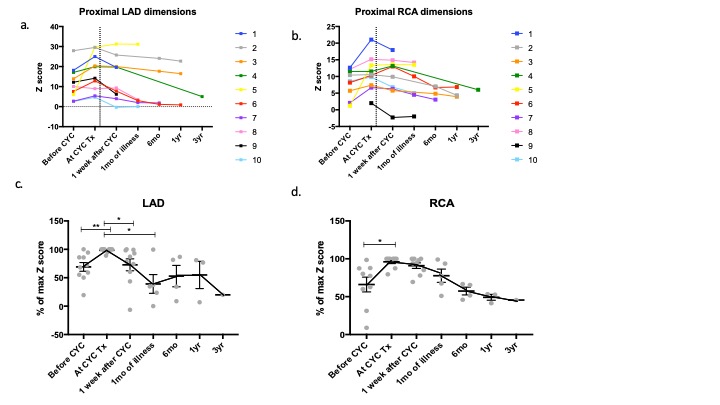
c, d, Normalized z scores of LAD and RCA dimensions. The data expressed as a percentage of highest Z score value per patient with highest equal 100%. Each dot represents individual patient. *p<0.05, **p<0.005 in paired t_test.
*Left Anterior Descending Artery
**Right Coronary Artery
To cite this abstract in AMA style:
Halyabar O, Son M, Chang M, Sundel R. Cyclophosphamide Use in Treatment of Refractory Kawasaki Disease: A Single Center Case Series of 10 Patients and Literature Review [abstract]. Arthritis Rheumatol. 2020; 72 (suppl 4). https://acrabstracts.org/abstract/cyclophosphamide-use-in-treatment-of-refractory-kawasaki-disease-a-single-center-case-series-of-10-patients-and-literature-review/. Accessed .« Back to 2020 Pediatric Rheumatology Symposium
ACR Meeting Abstracts - https://acrabstracts.org/abstract/cyclophosphamide-use-in-treatment-of-refractory-kawasaki-disease-a-single-center-case-series-of-10-patients-and-literature-review/