Session Information
Session Type: ACR Concurrent Abstract Session
Session Time: 2:30PM-4:00PM
Background/Purpose: The accurate interpretation of creatine kinase (CK) values is critical as this laboratory measure guides the workup of suspected myopathies. Incidentally discovered CK elevation is a common reason for rheumatology referral. This study comprehensively evaluated clinical factors associated with CK levels among a nationally representative sample and determined the distribution of CK levels in race-ethnicity subgroups.
Methods: Data was analyzed from the cross-sectional National Health and Nutrition Examination Survey (NHANES) 2011-2014, which interviews and examines a representative sample of the U.S. population. Included subjects were non-pregnant adults ≥ 20 years old. Race-ethnicity was based on self-report. In analyses stratified by sex, linear and logistic regression was used to identified clinical variables associated with CK levels and the likelihood of an individual being outside of sex-specific reference ranges. To assess the role of muscle mass on race-ethnicity differences in CK, linear models were adjusted for body mass index (BMI), arm circumference, and waist circumference. In order to inform the appropriate upper limit of normal reference range, 95th percentiles of CK in sex/race-ethnicity subgroups were calculated, excluding patients with strenuous exercise in the past 3 days.
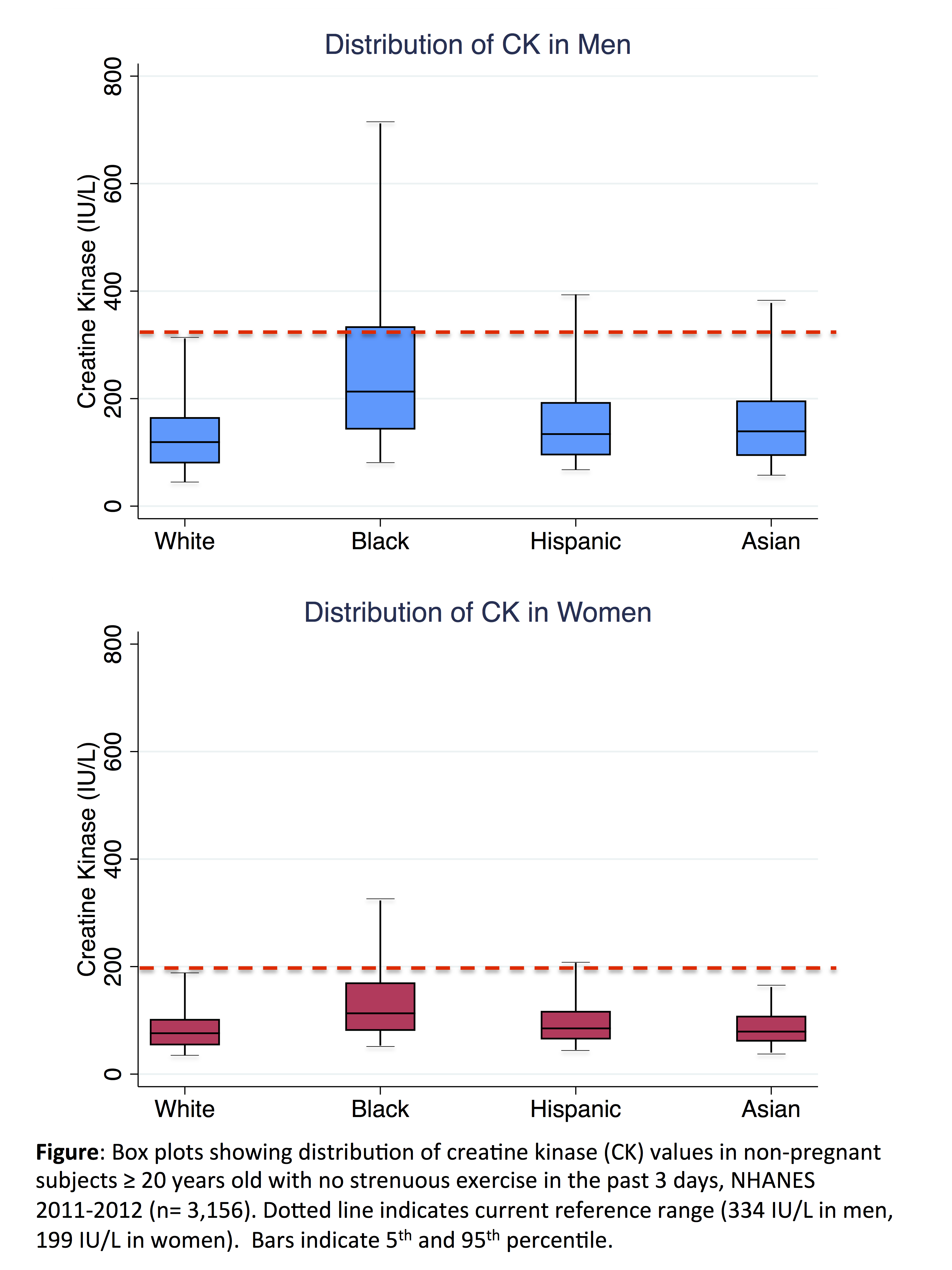
Results: A total of 10,096 subjects were included: 4119 non-Hispanic white, 2256 non-Hispanic black, 2159 Hispanic and 1270 Asian subjects. In linear and logistic regression, race-ethnicity was most strongly associated with CK among men and women. Compared to white subjects, CK was more likely to be abnormal in black men (OR 8.39, 95% CI 6.11 to 11.52) and in black women (OR 5.08, 95% CI 3.65 to 7.08). Greater BMI, chronic kidney disease, recent exercise, and physical activity were modestly associated with elevated CK, while men ≥ 70 were less likely to have an elevated CK (Table). Race-ethnicity differences in CK remained after adjustment for BMI, waist circumference, and arm circumference. The 95th percentile of CK was 312 (95% CI 268 to 356) in white men, 712 (95% CI 530 to 894) in black men, 188 (95% CI 122 to 254) in white women, and 323 (95% CI 218 to 428) in black women (Figure).
Conclusion: Creatine kinase values in the general population are substantially higher in black patients particularly among men. These racial differences are not explained by differences in body composition. Proposed reference ranges for race-specific subgroups in this study are markedly higher than current reference ranges and provide a practical guide for clinicians when interpreting CK values.
| Table: Multivariable logistic regression of odds of having creatine kinase above the upper limit of normal (334 IU/L in males, 199 IU/L in females) | ||
|
Male OR (95% CI) abnormal CK |
Female OR (95% CI) abnormal CK |
|
| Race-ethnicity (vs. White) |
|
|
| Black |
8.39 (6.11,11.52)*** |
5.08 (3.65,7.08)*** |
| Hispanic |
1.72 (1.26,2.34)** |
1.20 (0.83,1.73) |
| Asian |
2.41 (1.58,3.66)*** |
1.18 (0.68,2.03) |
| Other |
1.78 (0.82,3.85) |
1.59 (0.65,3.87) |
| Age (vs. 20-29 years old) |
|
|
| 30-49 |
0.97 (0.70,1.34) |
0.69 (0.41,1.15) |
| 50-69 |
0.52 (0.30,0.90)* |
0.66 (0.36,1.23) |
| ≥ 70 |
0.26 (0.11,0.60)** |
0.55 (0.25,1.20) |
| BMI (vs. 20-25 kg/m2) |
|
|
| < 18.5 |
0.55 (0.23,1.48) |
0.20 (0.05,0.75)* |
| 25-30 |
2.29 (1.67,3.13)*** |
1.16 (0.75,1.79) |
| ≥ 30 |
2.52 (1.80,3.54)*** |
1.11 (0.72,1.70) |
| GFR (vs. ≥ 90 ml/min/1.73m2) |
|
|
| 60-89 |
1.56 (1.22,1.99)** |
1.60 (1.10,2.32)* |
| 30-59 |
2.21 (0.99,4.92) |
2.06 (1.18,3.60)* |
| <30 |
0.44 (0.07,2.88) |
1.00 (0.30,3.34) |
| Exercise in past 3 days |
1.78 (1.27,2.50)** |
1.55 (0.89,2.68) |
| Vigorous recreation |
1.49 (1.13,1.95)** |
1.47 (0.97,2.23) |
| Heavy alcohol use, thyroid disease, hypertension, smoking, diabetes, cholesterol medication use, vigorous work included but not shown with p > 0.05 in men and women. BMI = body mass index. GFR = glomerular filtration rate. * < 0.05, ** < 0.01, *** < 0.001 | ||
To cite this abstract in AMA style:
McGill NK, Baker JF, George MD. Creatine Kinase in the United States Population: Impact of Demographics, Comorbidities and Body Composition on the Normal Range [abstract]. Arthritis Rheumatol. 2016; 68 (suppl 10). https://acrabstracts.org/abstract/creatine-kinase-in-the-united-states-population-impact-of-demographics-comorbidities-and-body-composition-on-the-normal-range/. Accessed .« Back to 2016 ACR/ARHP Annual Meeting
ACR Meeting Abstracts - https://acrabstracts.org/abstract/creatine-kinase-in-the-united-states-population-impact-of-demographics-comorbidities-and-body-composition-on-the-normal-range/