Session Information
Session Type: Abstract Submissions (ACR)
Background/Purpose: Glucocorticoids (GC) are among the most effective drugs in rheumatoid arthritis (RA), but concerns over long-term side effects have not been resolved. Recent studies indicate that cumulative exposure to GC is associated with an increased risk of cardiovascular (CV) disease, perhaps in part through worsening of the CV risk profile. However, GC also strongly decrease inflammation in RA, and inflammation also has an etiological role in the increased CV risk in this group. The net effect of GC use on CV risk in RA therefore remains unknown.
Methods: RA patients aged 50-75 years were followed for approximately 10 years to study the development of CV disease in the Cardiovascular Risk in RhEumatoid arthritis (CARRE) study. This study was the first to report that CV disease incidence in RA was equal to diabetes mellitus. For the current study, GC exposure was characterized by duration, last exposure by date, the mean dose of GC and cumulative exposure in grams. Data collection included traditional CV risk factors and RA-related parameters and disease activity. Cox proportional hazard analysed the association between GC exposure and incident CV disease, with adjustment for confounders.
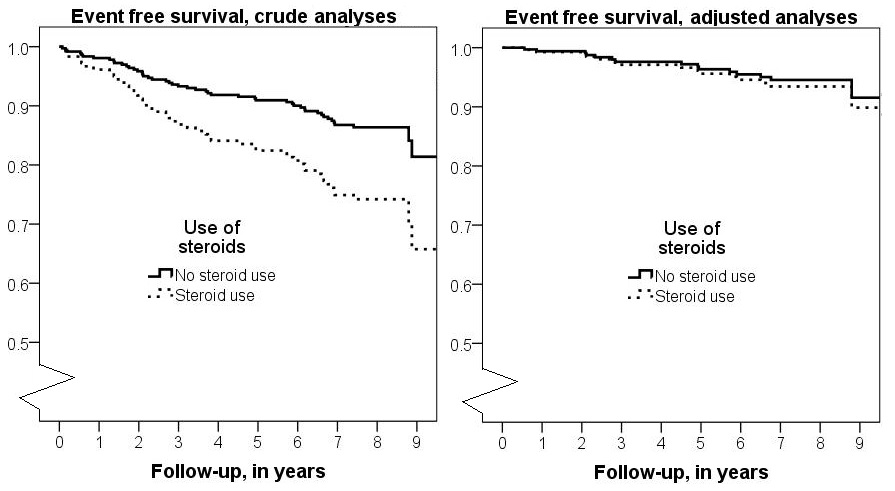
Results: The study comprised 353 individuals of whom 59 (17%) were exposed to GC at the time of inclusion, with a median (interquartile range) the cumulative exposure was 8.7 (2.5-25.4) grams. After a total follow-up experience of 2361 years, 58 (17%) participants developed incident CV disease, yielding an incidence rate of 24.6/1.000 patient years. Incident cases were more frequently treated with GC at baseline than RA patients without CV disease (22 vs. 16%, p-value 0.089), were treated with GC for a longer period (4.1 vs. 1.9 years, p-value 0.090) and cumulatively used more GC (31.9 vs. 8.5 grams, p-value 0.046). These differences remained after adjustment for demographics and CV risk. However, additional adjustment for at baseline measured 28-joint disease activity score (DAS28) and disability (Health Assessment Questionnaire, HAQ) completely erased the associations of GC with incident CV disease. These observations appear robust and unaffected by power constraints, as the standard errors of the beta estimates remained essentially similar after adjustment.
Conclusion: It appears that GC use in uncontrolled populations represents a marker of high RA disease activity; high disease activity itself represents an increased risk of CV disease. Thus the observed relationship of GC with CV disease in RA patients is strongly confounded by indication, as suggested by the adjusted analyses. In this setting, it is possible that the adverse CV effects of GC are balanced by positive effects working through inflammation control.
Figure. Kaplan-Meier survival curves
Disclosure:
A. M. van Sijl,
None;
M. Boers,
None;
A. E. Voskuyl,
None;
M. T. Nurmohamed,
None.
« Back to 2013 ACR/ARHP Annual Meeting
ACR Meeting Abstracts - https://acrabstracts.org/abstract/confounding-by-indication-distorts-the-relationship-between-steroid-use-and-cardiovascular-disease-in-rheumatoid-arthritis/