Genome-wide association studies suggest that PR3-ANCA-positive ANCA-associated vasculitis (AAV) is genetically distinct from MPO-ANCA AAV. We evaluated patients enrolled in the RAVE trial according to ANCA type (PR3- versus MPO-ANCA) as opposed to disease type (granulomatosis with polyangiitis [GPA] versus microscopic polyangiitis [MPA]) to explore whether either classification predicts clinical course and response to treatment
Methods
The RAVE trial randomized 197 patients to receive rituximab (RTX) or CYC followed by AZA (CYC/AZA) for remission induction. Demographics, clinical features, response to induction treatment, and disease flares were analyzed according to ANCA type and AAV diagnosis. Chi square, Fisher and Mann-Whitney tests were used for univariate analyses. Logistic regression was used for multivariate analyses
Results
Demographic characteristics and baseline organ system involvement: Considerable overlap existed between ANCA type and AAV diagnosis with regard to patient demographics and clinical phenotype (Table 1). Patients with GPA and PR3 were younger, more often male, and had more constitutional, ocular and ENT manifestations compared to those with MPA and MPO. Renal disease was more common among patients with MPA and MPO
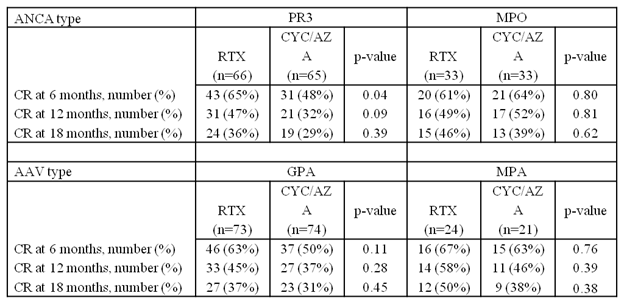
Response to treatment: PR3-positive patients achieved complete remission (CR) at 6 months more frequently when treated with RTX (65%) than CYC/AZA (48%) (p = 0.04) (Table 2). Findings were consistent after adjustments for age, sex and new versus relapsing disease. No significant association between CR at 6 months and treatment allocation was seen for MPO patients. When stratified by AAV diagnosis, the proportion of patients in CR at 6 months was not significantly different between treatment arms. The difference in response to treatment was no longer seen at 12 and 18 months, by which time the effects of RTX had waned
Disease relapse: A higher percentage of PR3 and GPA patients had experienced flares at 12 and 18 months than did their MPO and MPA counterparts. There were no differences in time to first flare
Conclusion
PR3-positive patients were more likely to achieve CR at 6 months if treated with RTX than with CYC/AZA. This observation requires confirmation in future studies but supports the concept that classifying patients according to ANCA type rather than AAV diagnosis may be highly relevant to the choice of remission induction therapy. Patient demographics, clinical features, and disease relapse were similar when patients were stratified by either AAV diagnosis or ANCA type
Table 1 Baseline characteristics
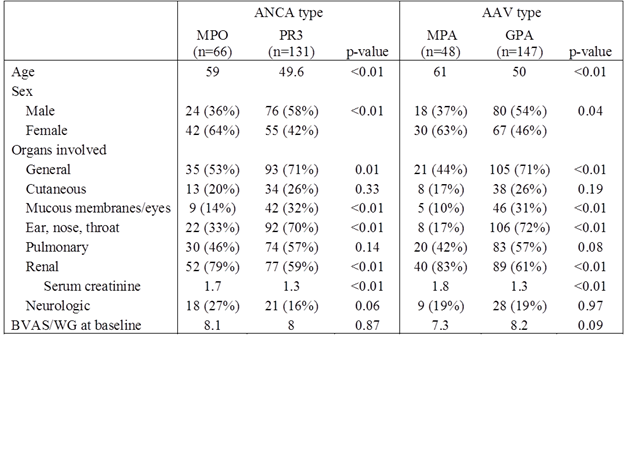
Table 2 Treatment response
Disclosure:
S. Unizony,
None;
E. M. Miloslavsky,
Genentech and Biogen IDEC Inc.,
5;
M. Villarreal,
None;
P. A. Merkel,
Genentech and Biogen IDEC Inc.,
2,
Bristol-Myers Squibb,
2,
GlaxoSmithKline,
2,
Actelion Pharmaceuticals US,
2,
Actelion Pharmaceuticals US,
5,
Sanofi-Aventis Pharmaceutical,
5,
Chemocentryx,
5;
P. Monach,
None;
E. W. St. Claire,
None;
C. Kallenberg,
None;
D. Ikle,
None;
R. F. Spiera,
roche-genetech,
2;
N. Tchao,
None;
D. J. Phippard,
None;
L. Ding,
None;
C. A. Langford,
Genentech and Biogen IDEC Inc.,
2;
P. Seo,
None;
G. S. Hoffman,
None;
J. H. Stone,
None;
U. Specks,
None.
« Back to 2014 ACR/ARHP Annual Meeting
ACR Meeting Abstracts - https://acrabstracts.org/abstract/comparison-of-clinicopathologically-and-serologically-based-classification-systems-for-anca-associated-vasculitis/