Session Information
Date: Monday, November 9, 2015
Session Type: ACR Poster Session B
Session Time: 9:00AM-11:00AM
Background/Purpose: The incidence of Clostridium difficile infection (CDI)
has increased among children, and CDI is associated with significant morbidity
and mortality. Cases of C. difficile infection-associated reactive arthritis (CDIAREA) in
children have been described, but the epidemiology of this complication is
poorly understood.
Methods: We performed a descriptive cohort and
nested case-control study of CDIAREA in individuals aged 2-20 years using the
electronic medical record of two large pediatric care networks from 2004-2013.
Cases of CDIAREA were defined as presence of acute arthritis and/or
tenosynovitis between ²4 weeks before and ³12 weeks after confirmed,
symptomatic CDI with 1) no other apparent cause for arthritis and 2) negative
synovial cultures (if obtained). Each case was compared to up to 4 controls
with CDI without arthritis/tenosynovitis, randomly selected at the time of
CDIAREA diagnosis ±3 months, using conditional logistic regression. Incidence
of CDIAREA was calculated based on cases and unaffected children seen as an
outpatient in the respective care network within the last 2 years. Attack rate
was calculated as cases of CDIAREA per total number of CDIs during the same
time period.
Results: We identified 26 cases of CDIAREA
during the study period, with an incidence of 5.0 cases
per million person-years (95% CI 3.0, 7.8) and an attack rate of 6.4 cases per
1000 CDIs (95% CI 3.6, 10.5). Among cases of CDIAREA, the acute onset of joint
symptoms began a median of 11 days (IQR 7, 15) after gastrointestinal symptom
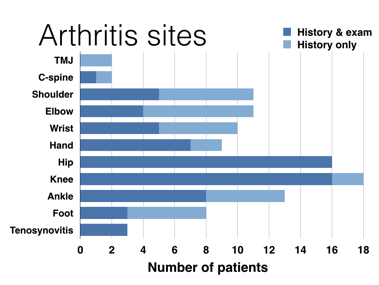
onset. CDIAREA typically involved multiple joints (median 5, IQR 3, 8) in
migratory fashion (77%), most commonly the hip and knee (Figure). About half of
children with CDIAREA had fever (58%) or rash (54%). Among those with CDIAREA,
5 (19%) were treated for a presumed septic hip arthritis even though all had
negative synovial cultures. All cases with CDIAREA and presumed septic hip
arthritis had post-antibiotic diarrhea and/or other joints affected before
surgical drainage. Not including those with hospital-onset CDI, cases with
CDIAREA were more commonly treated in the emergency room and/or hospitalized
(P=0.02), despite having fewer comorbidities and more community-onset CDI
(Table). Treating providers made a diagnosis of CDIAREA in only 36% of cases
(95% CI 18%, 57%).
Conclusion: CDIAREA is an acute, under-recognized,
potentially morbid reactive arthritis associated with C. difficile infection that is often
confused with septic arthritis. Better recognition of CDIAREA in children is
needed.
Figure. Joint
involvement for children with C. difficile infection-associated reactive arthritis.
|
Table. Characteristics of children with C. difficile infection-associated reactive arthritis and controls with C. difficile infection without arthritis |
|||
|
Characteristic
|
Cases (N=26)
|
Controls (N=94)
|
P-valuea
|
|
Age, median (IQR) |
8 (6, 14) |
8 (3, 13) |
0.28 |
|
Female sex, N (%) |
13 (50) |
45 (48) |
0.75 |
|
Race, N (%) White Black Other
|
19 (73) 3 (12) 4 (15) |
68 (72) 18 (19) 8 (9) |
0.39b |
|
Number of medical comorbidities, median (IQR) |
0 (0, 1) |
1 (1, 2) |
0.01 |
|
Autoimmune comorbidity, N (%) |
3 (12) |
16 (17) |
0.58 |
|
Prior C. diff infection, N (%) |
1 (4) |
10 (11) |
0.38 |
|
Antibiotic exposure in prior 2 months, N (%) |
22 (85) |
78 (84) |
0.90 |
|
Community-onset C. diff infectionc, N (%) |
26 (100) |
69 (74) |
0.004b |
|
Hospitalized, N (%) Hospitalized for C. diff symptoms or dehydration Hospitalized for arthritis Hospitalized for other reason
|
21 (81) 6 (23) 17 (65) 0 |
51 (55) 27 (29) 0 24 (36) |
0.02 0.77 – – |
|
Seen in emergency room and/or hospitalized (any reason) |
24 (92) |
60 (64) |
0.02 |
|
Seen in emergency room and/or acutely hospitalized for C. diff infection-related illnessd, N (%) |
24 (92) |
36 (38) |
0.001 |
|
a P-values were obtained from conditional logistic regression model. b P-value signifies overall chi-square. c Symptom onset outside of the hospital or before hospital day 3. d Hospitalization for abdominal symptoms, dehydration, or arthritis, not including prior hospitalization leading to hospital-associated C. difficile infection. |
|||
To cite this abstract in AMA style:
Horton DB, Strom BL, Putt ME, Rose CD, Sherry DD, Sammons JS. Clostridium Difficile Infection-Associated Reactive Arthritis in a Pediatric Cohort [abstract]. Arthritis Rheumatol. 2015; 67 (suppl 10). https://acrabstracts.org/abstract/clostridium-difficile-infection-associated-reactive-arthritis-in-a-pediatric-cohort/. Accessed .« Back to 2015 ACR/ARHP Annual Meeting
ACR Meeting Abstracts - https://acrabstracts.org/abstract/clostridium-difficile-infection-associated-reactive-arthritis-in-a-pediatric-cohort/