Session Information
Session Type: Poster Session (Monday)
Session Time: 9:00AM-11:00AM
Background/Purpose: Gout is the most common inflammatory arthritis in the United States and worldwide. Precipitation of monosodium urate crystals in joints and soft tissues leads to inflammation and the clinical signs and symptoms of gout. Identification of urate crystals on synovial fluid analysis remains the gold standard for diagnosis. However, arthrocentesis is not always a viable option, particularly if the patient presents without active inflammation or effusion on exam. Dual energy computed tomography (DECT) is another tool for noninvasive diagnosis of gout and can be utilized in the acute or chronic stages. The 2015 American College of Rheumatology (ACR) and the European League Against Rheumatism (EULAR) classification criteria for gout recognize a role for DECT in diagnosis. In our retrospective study, we analyzed how DECT is utilized in a cohort of patients at Mayo Clinic in Jacksonville, Florida. We sought to determine better clinical parameters for ordering DECT in our rheumatology department.
Methods: Our retrospective study was approved by the institutional review board. Informed consent was waived due to the retrospective nature of the study. DECT scans performed from January 2010 to April 2018 were identified using radiology software by a board certified, fellowship trained radiologist with expertise in musculoskeletal imaging. Lower extremity, upper extremity, and spine DECT were included.
Results: 228 DECT were ordered over the observation period. Rheumatology accounted for the highest percentage (60%) of tests ordered, followed by primary care physicians (18%). 211 studies were requested to aid in the initial diagnosis of the patient’s concern with 129 ordered by rheumatology. Whereas the number of scans ordered by other departments changed little over the eight year observation period, DECT studies, ordered by rheumatology, decreased from 2015 onward. DECT was positive for urate 53% of the time (68 of 129) when ordered for initial diagnosis by rheumatology. Arthrocentesis was attempted on 15 patients to establish a diagnosis of gout. No synovial fluid was obtained from 10 of 15 patients. 80% of these patients had DECT performed which positively identified urate crystals. The other 5 patients, who underwent arthrocentesis, had synovial fluid examined by microscopy with 4 of 5 identifying no crystals. One patient with negative fluid analysis underwent repeat arthrocentesis showing positively birefringent rhomboid crystals. One patient with no crystals on microscopy had a positive DECT scan. Ultrasound (US) was performed on 6 patients in the clinic by the rheumatologist prior to DECT imaging. Double contour sign was identified on each patient. DECT confirmed the diagnosis of gout in these six patients.
Conclusion: The utilization of DECT in gout diagnosis is likely to continue to increase given that it is noninvasive, an accepted criterion in the ACR/EULAR 2015 guidelines, and more readily available. Our study highlights that DECT can be a useful tool in gout diagnosis when there is diagnostic uncertainty, no active inflammation or effusion on exam, and arthrocentesis cannot be obtained. Though the cohort was small, US can be a viable option as a noninvasive tool in gout diagnosis.

Figure 1
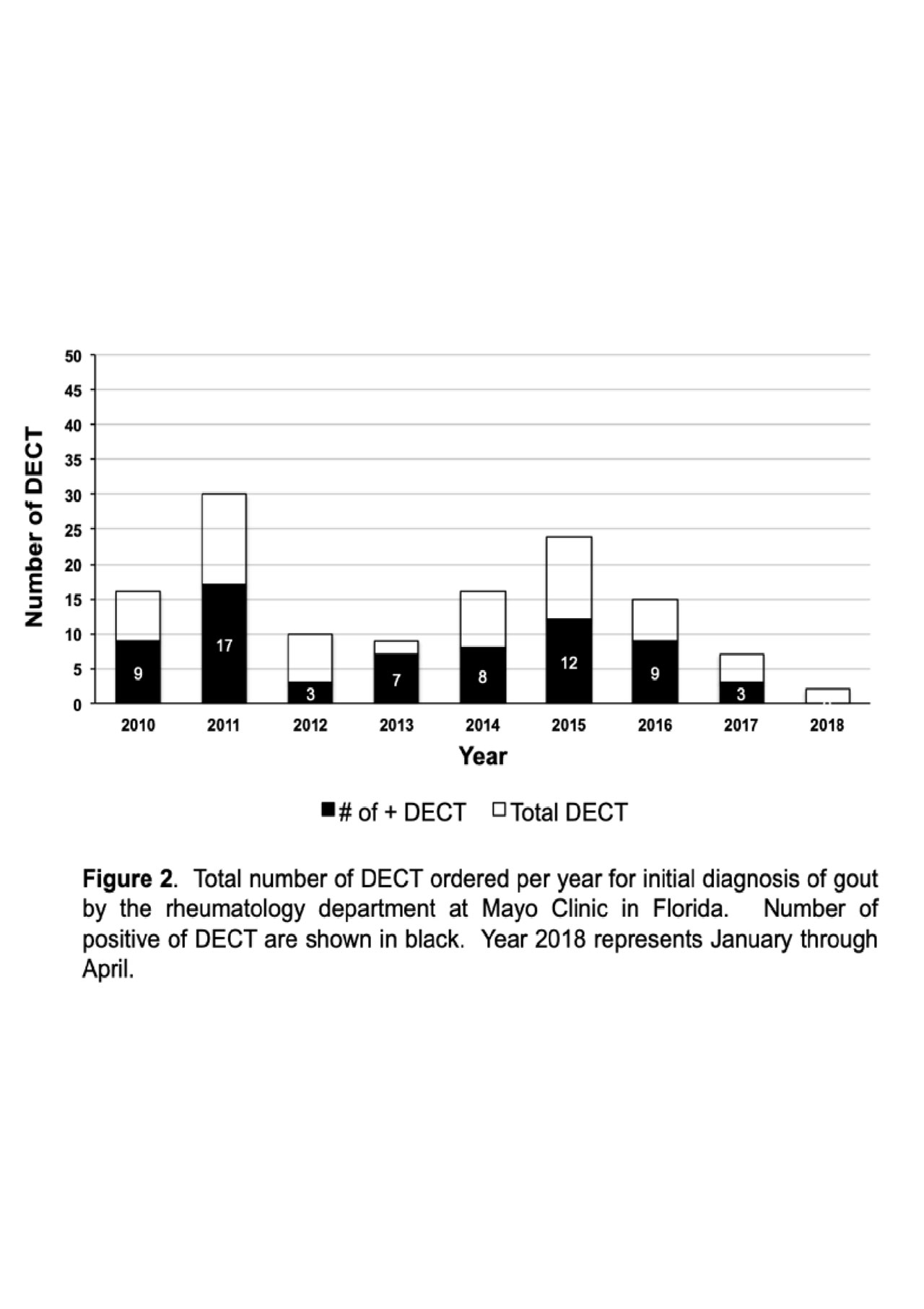
Figure 2
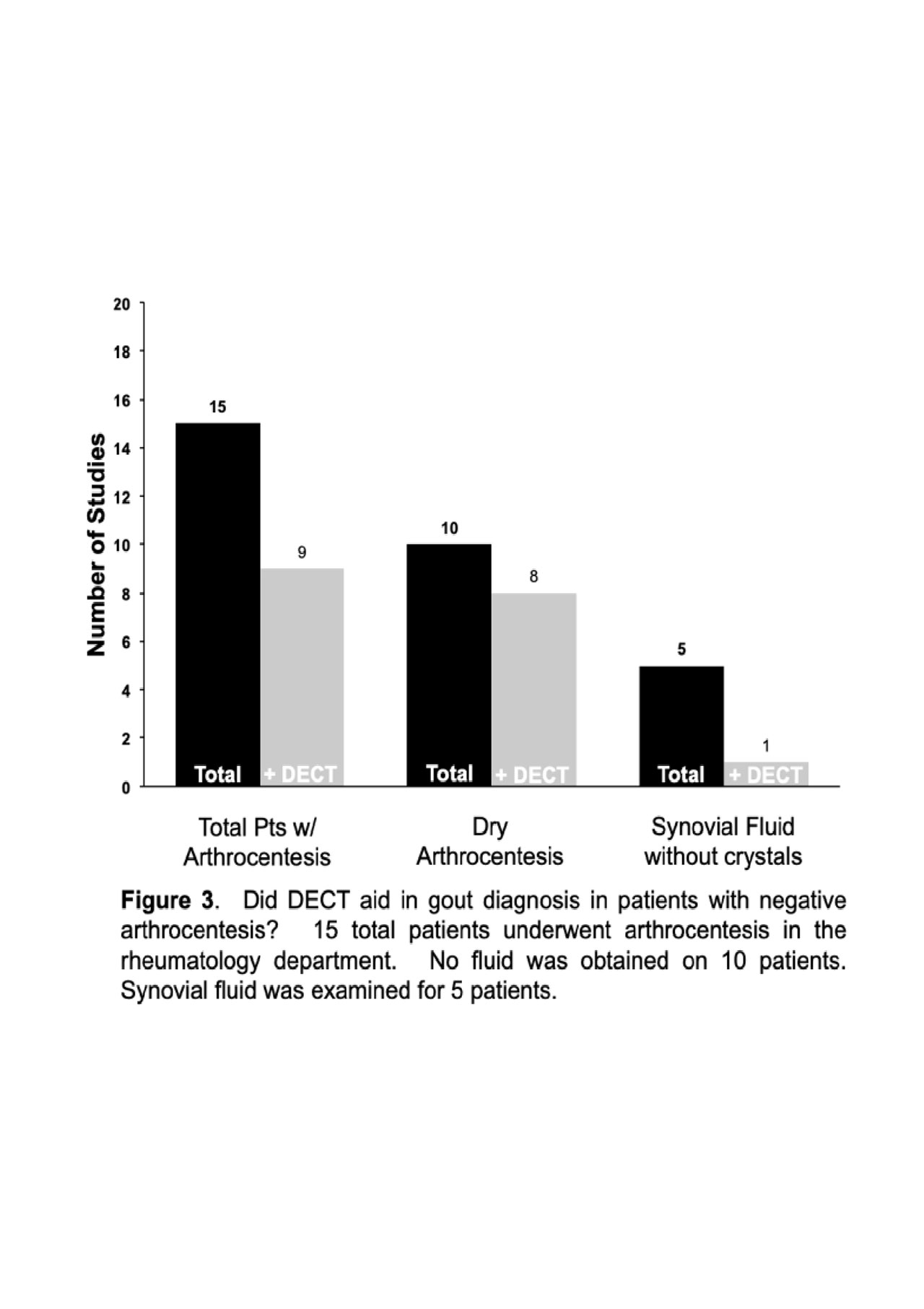
Figure 3
To cite this abstract in AMA style:
Gilbert E, Garner H, Abril A. Clinical Utility of DECT in the Diagnosis of Gout at Mayo Clinic in Florida [abstract]. Arthritis Rheumatol. 2019; 71 (suppl 10). https://acrabstracts.org/abstract/clinical-utility-of-dect-in-the-diagnosis-of-gout-at-mayo-clinic-in-florida/. Accessed .« Back to 2019 ACR/ARP Annual Meeting
ACR Meeting Abstracts - https://acrabstracts.org/abstract/clinical-utility-of-dect-in-the-diagnosis-of-gout-at-mayo-clinic-in-florida/