Session Information
Session Time: 5:00PM-6:00PM
Background/Purpose: Anti-synthetase syndrome (ASyS) is a rare autoimmune myopathy in children characterized by a triad of myositis, arthritis, and interstitial lung disease (ILD), though not all manifestations may be present at disease onset. Pediatric data remain limited, and disease presentation may differ from that in adults. We aim to describe the characteristics of pediatric patients with anti-synthetase antibodies at a large tertiary care center.
Methods: A retrospective review of children younger than 18 years with positive anti-synthetase antibodies seen at a large tertiary center between 2011 and 2024 was performed. The proposed classification criteria for anti-synthetase syndrome (CLASS) by the CLASS project was included. Demographics, clinical features, muscle enzymes, serologies, imaging studies, pulmonary function test (PFT) findings, and medication use were collected. Descriptive statistics are summarized.
Results: Eight patients (all female) met the inclusion criteria. The mean age at diagnosis was 11.5 years. Two patients presented with the classic triad of myositis, arthritis, and ILD. Only one patient had mechanic’s hands. None presented with prolonged fever. One patient who met probable criteria did not have a rheumatologic diagnosis and myositis resolved without treatment. Anti–Jo-1 was the most frequent anti-synthetase antibody (4/8), followed by anti–PL-12 antibody (2/8) (Table 1). Gottron’s papules, peripheral arthritis, proximal muscle weakness, and cough with shortness of breath were the most common presenting clinical symptoms (organ involvement is described in Table 2). Elevated muscle enzymes were seen in half of the patients at disease presentation. One had electromyography completed with evidence of myositis, and two had myositis confirmed by biopsy. PFTs were obtained in 7/8 patients; 4 patients had a restrictive pattern. Three of these had evidence of ILD on CT imaging: 2 with a non-specific interstitial pneumonia pattern and 1 without a specific pattern (Figure 2). The most common treatments used were steroids (7/8), hydroxychloroquine (6/8), methotrexate (5/8), IVIG (5/8), and rituximab (3/8). Remission was achieved in 4 patients with a mean time from treatment onset of 18.25 months. No patients with ILD achieved remission.
Conclusion: ASyS has a heterogeneous clinical presentation, often with the development of organ involvement during the disease course. ILD remains a concerning component with a poor response to treatment in our cohort. Given the progression of disease with potential for refractory ILD, early recognition is essential to enable timely evaluation and management. Additional research is needed to identify patients in whom early testing for anti-synthetase antibodies would be warranted and to study the effectiveness of treatment options. In future research, we aim to compare characteristics of patients with anti-synthetase antibodies with those of patients with non-anti-synthetase myositis and ILD.
Table 1. Patient Characteristics at Presentation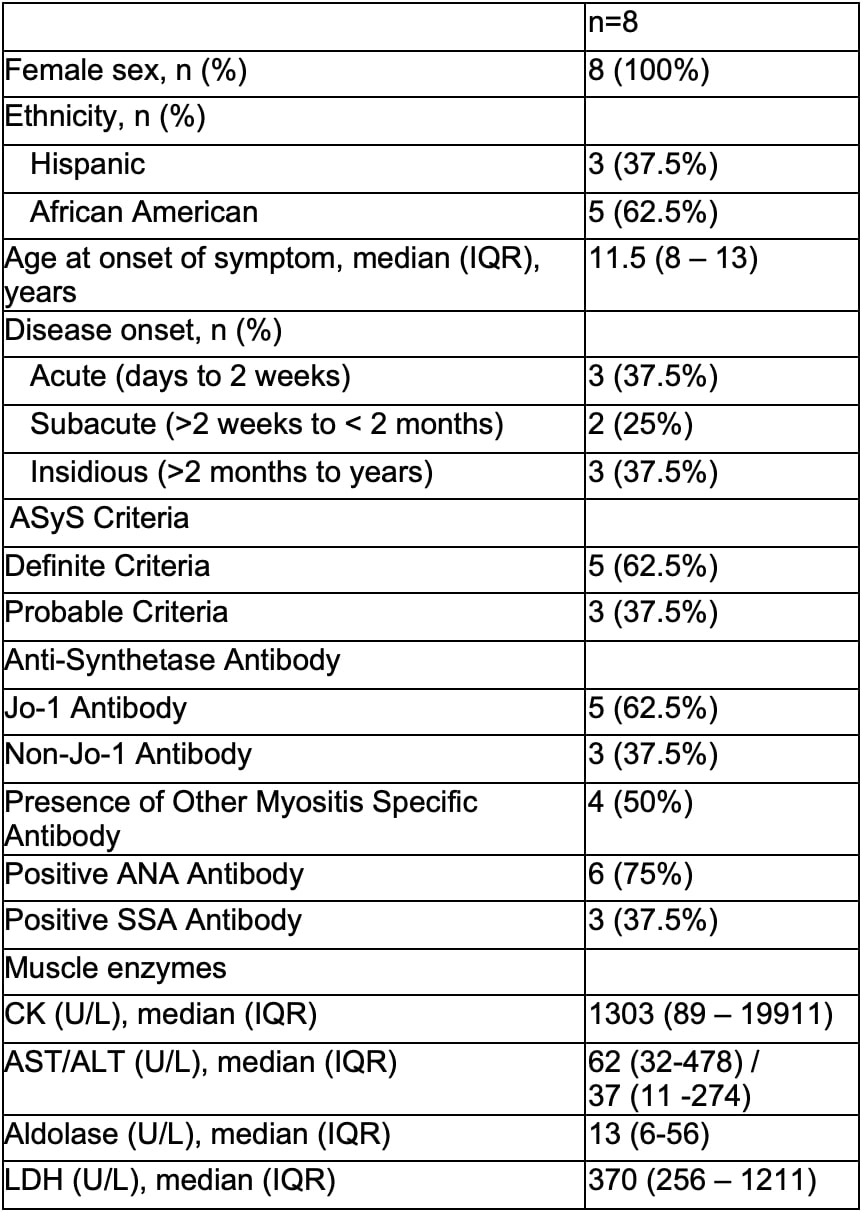
Table 2. Organ Involvement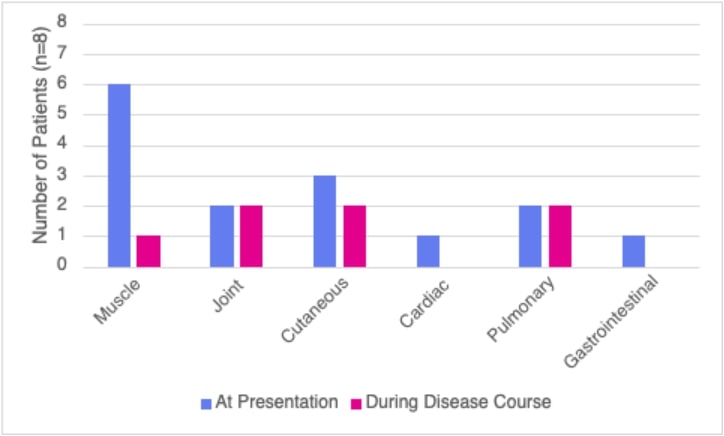 Muscle involvement includes clinical, MRI, EMG, laboratory, or biopsy evidence of myositis. Cutaneous involvement includes raynaud’s phenomenon, heliotrope rash, gottron’s papules, and mechanic’s hands. Cardiac involvement includes arrhythmia. Pulmonary involvement includes clinical symptoms, abnormal PFTs, and abnormal imaging. Gastrointestinal involvement includes dysphagia.
Muscle involvement includes clinical, MRI, EMG, laboratory, or biopsy evidence of myositis. Cutaneous involvement includes raynaud’s phenomenon, heliotrope rash, gottron’s papules, and mechanic’s hands. Cardiac involvement includes arrhythmia. Pulmonary involvement includes clinical symptoms, abnormal PFTs, and abnormal imaging. Gastrointestinal involvement includes dysphagia.
Figure 1 (A-D). Radiologic findings in a patient with Jo-1 Interstitial Lung Disease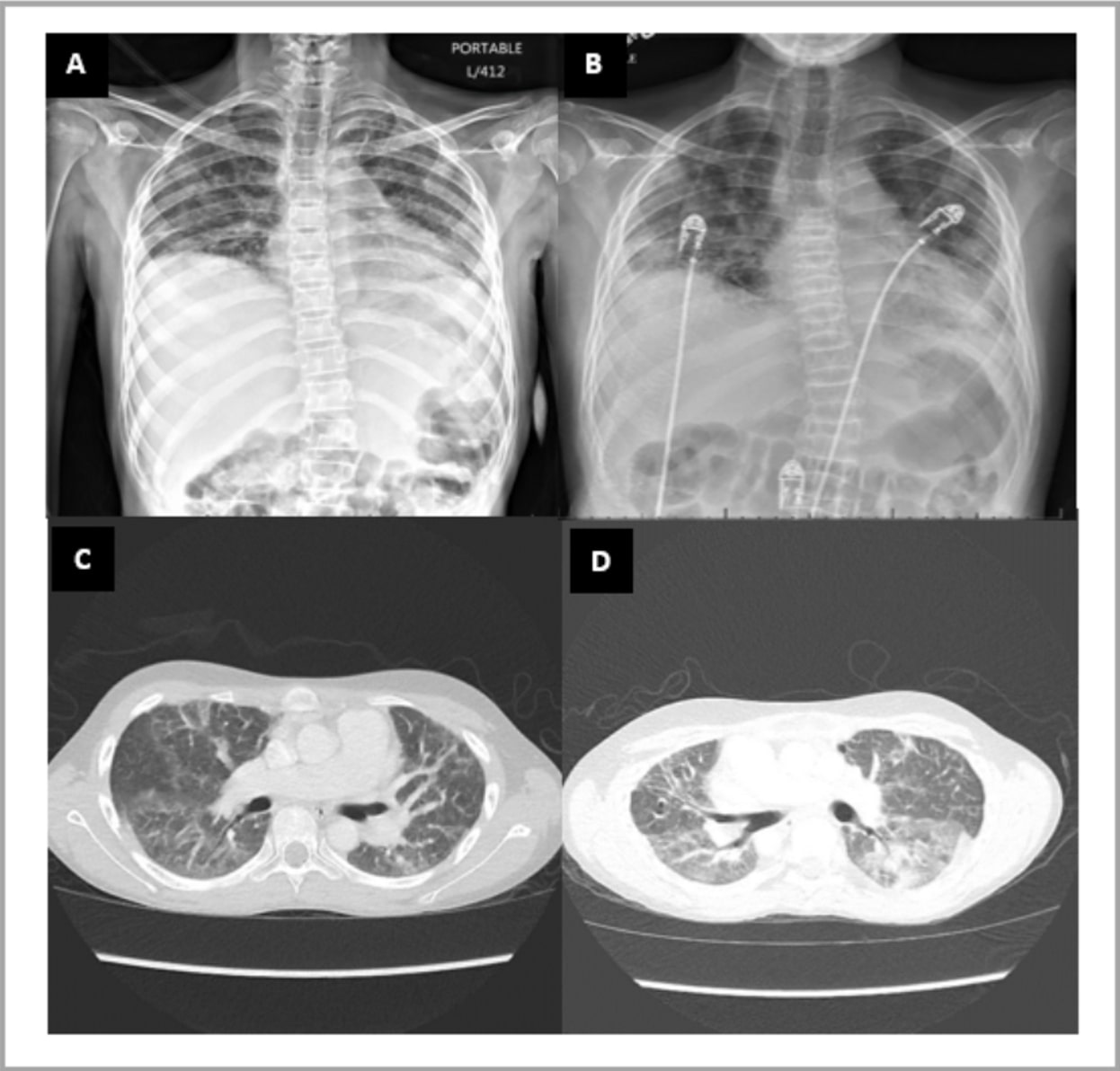 Chest radiograph (A and B) and CT Chest without contrast (C and D). Images show low lung volumes, multifocal bilateral ground glass opacities, more pronounced at the lung bases. Findings supportive of nonspecific interstitial pneumonia. Note the architectural distortion/fibrosis throughout both lungs and bone demineralization with multilevel vertebral body compression fractures developed over time.
Chest radiograph (A and B) and CT Chest without contrast (C and D). Images show low lung volumes, multifocal bilateral ground glass opacities, more pronounced at the lung bases. Findings supportive of nonspecific interstitial pneumonia. Note the architectural distortion/fibrosis throughout both lungs and bone demineralization with multilevel vertebral body compression fractures developed over time.
To cite this abstract in AMA style:
Marrs J, Correa M, Silva-Carmona M, Pereira M. Clinical Features of Juvenile Antisynthetase Syndrome: A Single-Center Case Series [abstract]. Arthritis Rheumatol. 2026; 78 (suppl 3). https://acrabstracts.org/abstract/clinical-features-of-juvenile-antisynthetase-syndrome-a-single-center-case-series/. Accessed .« Back to 2026 Pediatric Rheumatology Symposium
ACR Meeting Abstracts - https://acrabstracts.org/abstract/clinical-features-of-juvenile-antisynthetase-syndrome-a-single-center-case-series/