Session Information
Date: Tuesday, November 12, 2019
Title: Systemic Sclerosis & Related Disorders – Clinical Poster III
Session Type: Poster Session (Tuesday)
Session Time: 9:00AM-11:00AM
Background/Purpose: Mixed connective tissue disease (MCTD) is defined by presence of anti-RNP antibody together with 3 or more of swollen hands, synovitis, myositis, Raynaud phenomenon or acrosclerosis. Patients who fulfil diagnosis of SSc and have features of other connective tissue diseases are often classified as SSc-overlap. Our study aims to describe the clinical characteristics and outcomes of SSc-MCTD and SSc-overlap.
Methods: We included patients from the Australian Scleroderma Cohort Study (ASCS) who met ACR/EULAR diagnostic criteria for SSc. Three mutually exclusive groups were created: SSc-MCTD, SSc-overlap and SSc-only group (remaining patients). Univariate comparison of clinical features among groups was performed by ANOVA or chi-square. Survival analysis was performed using Kaplan-Meier curves, Wilcoxon test and Cox regression.
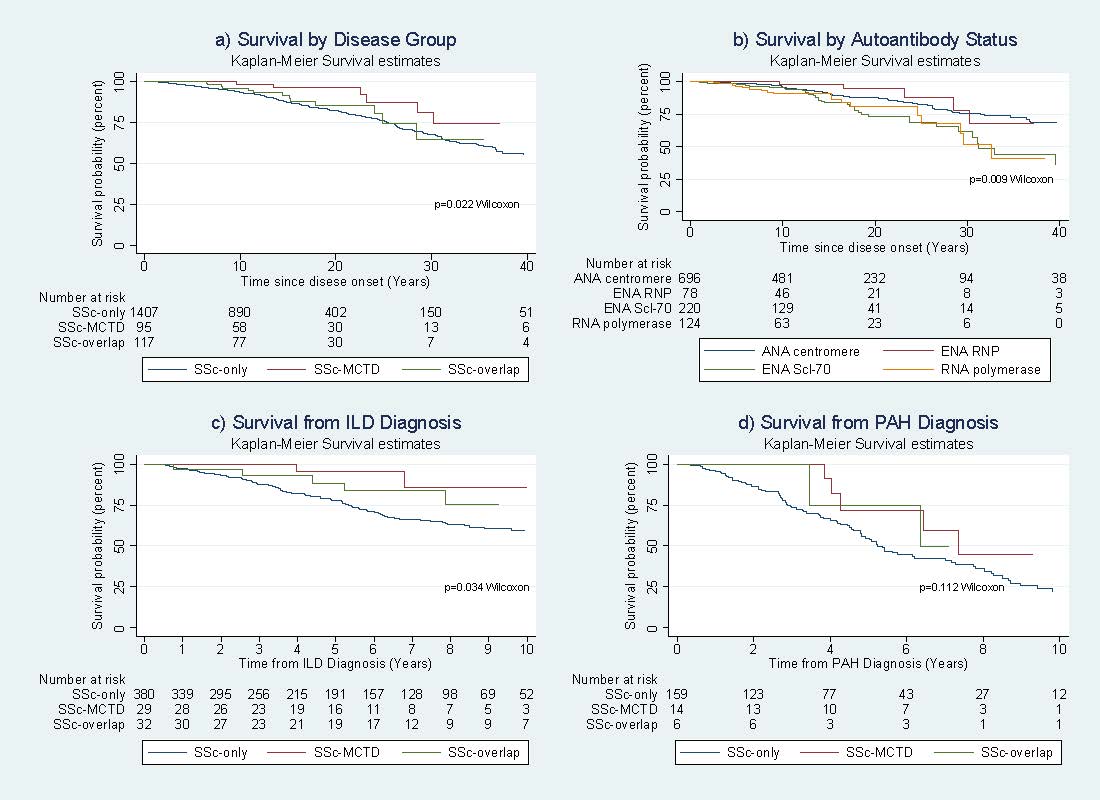
Results: Of 1728 patients, 102 (5.9%) had SSc-MCTD and 125 (7.2%) SSc-overlap. Those with MCTD-SSc were more commonly Asian (18.4% vs 9.3% in SSc-overlap and 3.6% in SSc-only, p< 0.0001). Those with SSc-MCTD or SSc-overlap were more likely to have limited SSc (81-84% vs. 73.1% for SSc-only). Both SSc-MCTD and SSc-overlap groups were more likely than SSc-only to have numerous positive autoantibodies such as anti-Ro, anti-Jo-1 and anti-Sm. SSc-MCTD and SSc-overlap had similar frequency of interstitial lung disease (ILD), while those with SSc-MCTD had higher frequency of pulmonary arterial hypertension (PAH) (13.7% vs 4.8% in SSc-overlap and 11% in SSc-only, p=0.0589). Synovitis and myositis were equally common in SSc-overlap and SSc-MCTD groups. SSc-MCTD or SSc-overlap conferred a higher likelihood of exposure to immunosuppression including prednisolone, synthetic and biologic DMARDs, than SSc-only . Overall survival was better in SSc-MCTD than SSc-overlap or SSc-only (Figure 1 a). However, scleroderma-specific antibodies were also survival prognostic markers, with ANA-centromere or anti-RNP conferring better survival than anti-Scl-70 or anti-RNA polymerase 3 (Figure 1 b). SSc-MCTD and SSc-overlap had lower all-cause mortality following diagnosis of ILD (Figure 1 c) and PAH than patients with SSc-only (Figure 1 d).
Conclusion: This study reveals significant clinical and survival differences between patients with SSc-MCTD, SSc-overlap and SSc-only. Importantly, despite higher frequency of PAH in SSc-MCTD, survival is better in SSc-MCTD and SSc-overlap than in SSc-only patients.
combine_for_abstract
To cite this abstract in AMA style:
Fairley J, Hansen D, Proudman S, Sahhar J, Ngian G, Walker J, Strickland G, Wilson M, Morrisroe K, Ferdowski N, Major G, Roddy J, Stevens W, Nikpour M. Clinical Characteristics and Survival in Systemic Sclerosis-mixed Connective Tissue Disease and Systemic Sclerosis-overlap Syndrome [abstract]. Arthritis Rheumatol. 2019; 71 (suppl 10). https://acrabstracts.org/abstract/clinical-characteristics-and-survival-in-systemic-sclerosis-mixed-connective-tissue-disease-and-systemic-sclerosis-overlap-syndrome/. Accessed .« Back to 2019 ACR/ARP Annual Meeting
ACR Meeting Abstracts - https://acrabstracts.org/abstract/clinical-characteristics-and-survival-in-systemic-sclerosis-mixed-connective-tissue-disease-and-systemic-sclerosis-overlap-syndrome/