Session Information
Date: Tuesday, November 9, 2021
Title: Vasculitis – Non-ANCA-Associated & Related Disorders Poster II (1862–1888)
Session Type: Poster Session D
Session Time: 8:30AM-10:30AM
Background/Purpose: To compare the clinical characteristics and determine the reliability of a self-reported diagnosis of giant cell arteritis (GCA) or Takayasu’s arteritis (TAK) from an international, internet-based cohort.
Methods: Patients with GCA and TAK enrolled in an internet-based registry were included. Data provided by patients were collected through standardized forms, including type of vasculitis, symptoms, results of diagnostic testing, and medication use. The percentage of patients who met the 1990 American College of Rheumatology (ACR) classification criteria were calculated. For the 2012 Chapel Hill Consensus Conference (CHCC) definitions, age >50 years and report of a positive biopsy or imaging were used as surrogates for a diagnosis of GCA, and age < 50 years with diagnosis on imaging were used as surrogates for a diagnosis of TAK.
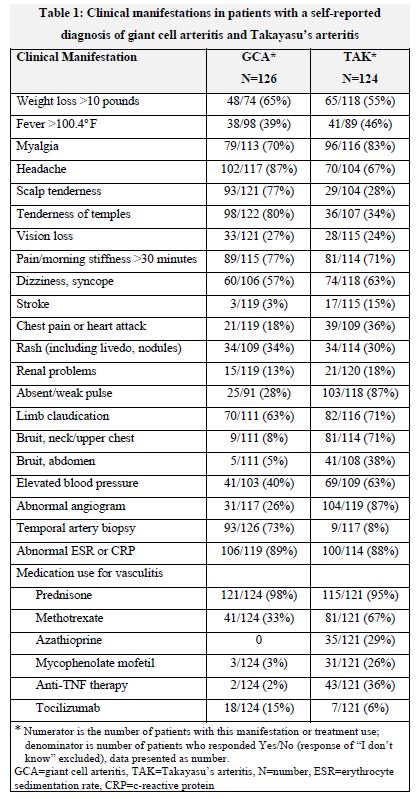
Results: The study included 250 patients with self-reported diagnoses (126 GCA and 124 TAK).
GCA cohort: The cohort was 80% female, mean (±SD) age 65 (±11.9) years. Mean (±SD) age at diagnosis of GCA was 62 (± 13.5) years. One patient aged 16 years was excluded. 9 patients (7%) reported age < 50 years old at the time of diagnosis (range 31 to 48 years). Of these, 2 patients had a temporal artery biopsy with 1 reported as positive in a 48 year-old. 93 patients (74%) reported having a temporal artery biopsy which was positive in 59 patients (63%). Abnormal imaging was reported in 39 patients (31%), 27 of whom also reported symptoms of limb claudication. The self-reported clinical symptoms of GCA are in Table 1. 87% met ACR classification criteria and 60% met the CHCC definition for GCA (93% met either, 87% met both).
TAK cohort: The cohort was 94% female, mean (±SD) age 42 (±15) years. Mean (±SD) age at diagnosis of TAK was 35 (±14.3) years. Twenty-six (21%) patients with TAK were ≥50 years at diagnosis, 15 patients (12%) with symptom onset at age ≥50 years. 97/112 patients (87%) reported blood pressure discrepancy in the upper extremities. Abnormal imaging was reported in 115 patients (93%). The self-reported clinical symptoms of TAK are outlined in Table 1.The subset of 26 patients ≥50 years old reported similar manifestations as the other patients with TAK, including abnormal angiogram (92%), limb claudication (77%), upper extremity blood pressure discrepancy (77%), bruits (77%). 95% of patients met ACR classification criteria. 75% met the CHCC definition for TAK; the majority who failed to meet the definition criteria did so on account of age. 96% patients met either ACR classification criteria or CHCC definition with 74% meeting both.
Conclusion: Patients with a self-reported diagnosis of GCA or TAK were able to reliably provide information about their symptoms and diagnosis. Clinical symptoms and treatments reported were consistent with what would be expected. The majority in both cohorts met ACR classification criteria or CHCC definitions. The high proportion of patients ≥50 years diagnosed as TAK likely reflects the uncertainty in clinical practice in this age group and classification by phenotype. These results provide support for the feasibility of conducting some types of research in these rare diseases through online registries.
To cite this abstract in AMA style:
Kermani T, Springer J, Shaw D, Young K, Burroughs C, Merkel P. Clinical Characteristics and Reliability of a Self-Reported Diagnosis of Large-Vessel Vasculitis [abstract]. Arthritis Rheumatol. 2021; 73 (suppl 9). https://acrabstracts.org/abstract/clinical-characteristics-and-reliability-of-a-self-reported-diagnosis-of-large-vessel-vasculitis/. Accessed .« Back to ACR Convergence 2021
ACR Meeting Abstracts - https://acrabstracts.org/abstract/clinical-characteristics-and-reliability-of-a-self-reported-diagnosis-of-large-vessel-vasculitis/