Session Information
Date: Sunday, November 12, 2023
Title: (0691–0721) Vasculitis – Non-ANCA-Associated & Related Disorders Poster I
Session Type: Poster Session A
Session Time: 9:00AM-11:00AM
Background/Purpose: Clinically isolated aortitis (CIA), or aortitis in the absence of identifiable systemic vasculitis, is typically discovered histopathologically after aortic aneurysm repair. The approach to caring for CIA patients as a rheumatologist remains uncertain, including the role of immunosuppression (IS) and the risk of developing systemic rheumatologic disease. To add to the limited literature on this topic1,2,we conducted a study using the Cardiovascular Health Improvement Project (CHIP) database at Michigan Medicine, which is enriched for patients with surgical aortic disease. Our aim was to identify and describe CIA patients in CHIP and provide insights into the clinical characteristics and outcomes.
Methods: We queried CHIP to identify patients with diagnosis codes or keywords in the electronic medical record (EMR) related to aortitis from 8/1/2013-3/31/2022. CIA cases were independently verified with chart review by two physicians. Patients without any follow-up in the EMR after diagnosis of aortitis were excluded. Clinical data was recorded at time of CIA diagnosis until date of last follow-up in EMR, including subsequent aortic events (subsequent aortic surgery, new or worsening aneurysm, new stenosis, or dissection).
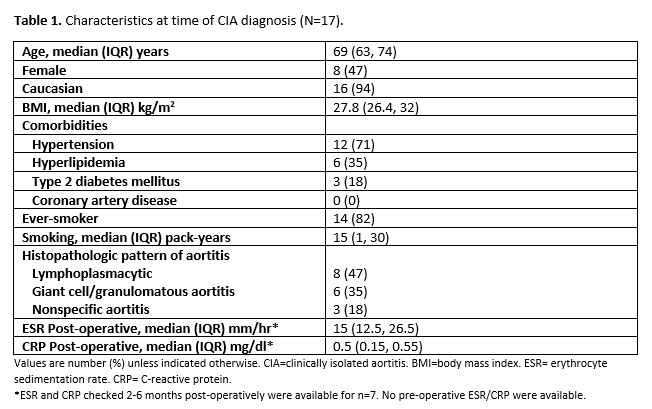
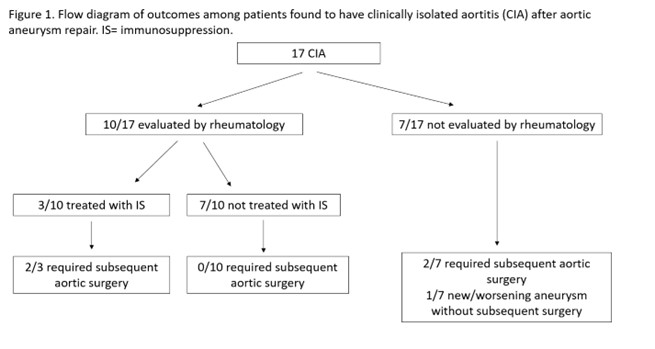
Results: 17 patients with CIA were identified with 7.1 (IQR 2.9, 10.0) years of follow-up, all of whom had undergone ascending aortic aneurysm repair. Clinical characteristics at CIA diagnosis are presented in Table 1. Rheumatology was engaged post-operatively in 10 cases (59%); only 3 patients (18%) were treated with IS (steroids ± tocilizumab) at any point during follow-up. One patient was diagnosed with systemic rheumatologic disease (rheumatoid arthritis) 6.6 years after CIA diagnosis. Subsequent aortic events occurred in 5 patients (29%) at median 3.7 (IQR 1.5, 6.2) years of follow-up (Figure 1). One patient passed due to unrelated reasons 16.4 years after CIA diagnosis.
Conclusion: In this single-center cohort of 17 patients with CIA aortic aneurysm repair, there was a high prevalence of hypertension and ever-smoking, and post-operative inflammatory markers (when available) tended to be normal. Interestingly, evolution into systemic rheumatologic disease was uncommon. A third of patients had subsequent aortic events after CIA diagnosis, highlighting the need for continued clinical surveillance of patients with CIA; no conclusions could be drawn regarding the impact of IS on preventing subsequent aortic events.
References:
1. Mayer A, Sperry A, Quimson L, Rhee R. Long-term clinical and radiographic outcomes in patients with clinically isolated aortitis. ACR Open 2022 Dec;4(12):1013-1020.
2. Clifford A, Arafat A, Idrees J et al. Outcomes among 196 patients with noninfectious proximal aortitis. Arth Rheum 2019 71(12):2112:2120.
To cite this abstract in AMA style:
Gewurz-Singer O, Ford J, Aung T, Humphrey-Stark L. Clinical Characteristics and Outcomes in Patients Found to Have Clinically Isolated Aortitis After Aortic Aneurysm Repair: A Single-Center Experience [abstract]. Arthritis Rheumatol. 2023; 75 (suppl 9). https://acrabstracts.org/abstract/clinical-characteristics-and-outcomes-in-patients-found-to-have-clinically-isolated-aortitis-after-aortic-aneurysm-repair-a-single-center-experience/. Accessed .« Back to ACR Convergence 2023
ACR Meeting Abstracts - https://acrabstracts.org/abstract/clinical-characteristics-and-outcomes-in-patients-found-to-have-clinically-isolated-aortitis-after-aortic-aneurysm-repair-a-single-center-experience/