Session Information
Session Time: 6:00PM-7:00PM
Background/Purpose: Pediatric chronic nonbacterial osteomyelitis (CNO) is a rare autoinflammatory bone disease that may co-occur with inflammatory bowel disease (IBD). Treatments for CNO may mask or exacerbate undiagnosed IBD. Early identification of IBD in CNO is critical to avoid diagnostic delays and optimize management. This study examines clinical features of CNO with and without IBD to identify distinguishing characteristics and guide screening.
Methods: A retrospective chart review (2007–2022) was conducted at Lurie Children’s Hospital using Epic and ICD-10 codes. The study was conducted prior to publication of the 2025 EULAR/ACR classification criteria for pediatric CNO. On review of the cohort, all patients with a diagnosis of CNO fulfilled all EULAR/ACR entry and exclusion criteria.
Data included age at onset, time to diagnosis, symptoms, growth, inflammatory markers, lesion distribution, biopsy, treatments, and imaging. For CNO/IBD patients, additional GI-related data was collected. Given the imbalance in group sizes, a bootstrap resampling method was used to provide robust estimates of the mean difference in numeric outcome variables of interest between the two groups. The Chi-Square test was conducted to explore bivariate associations between clinical factors in the CNO cohort. In instances with low counts, the Fisher-Exact test was applied for greater precision.
Results: A total of 95 patients were included, with descriptive and demographic data presented in Table 1. There were statistically significant differences in mean differences of time to MRI (mean difference = 362.9, CI (35.5, 613) and number of lesions (mean difference = -4.96, CI (-9.15, -.59). There were statistically significant differences in lesion location, platelet count, ESR, and fecal calprotectin. Lesion distribution by cohort is shown in Figure 1. Patients with CNO and IBD had higher frequency of thrombocytosis, elevated ESR, and abnormal fecal calprotectin compared to patients with CNO.
Conclusion: Despite a small sample size, the results suggest that patients with CNO and IBD exhibit more extensive bone lesions and systemic inflammation. A male predominance, multisite lesion distribution, and elevated inflammatory markers, especially fecal calprotectin, may signal underlying IBD. Fecal calprotectin should be used routinely as a screening lab in patients with CNO to improve earlier diagnosis of concurrent IBD. This study highlights diagnostic delays and supports the need for earlier whole-body MRI and GI referral in selected CNO cases. Bone biopsy remained common despite its limited diagnostic necessity in many cases. Multicenter studies are needed to validate these findings and improve early recognition of IBD in CNO.
Table 1: Descriptive Statistics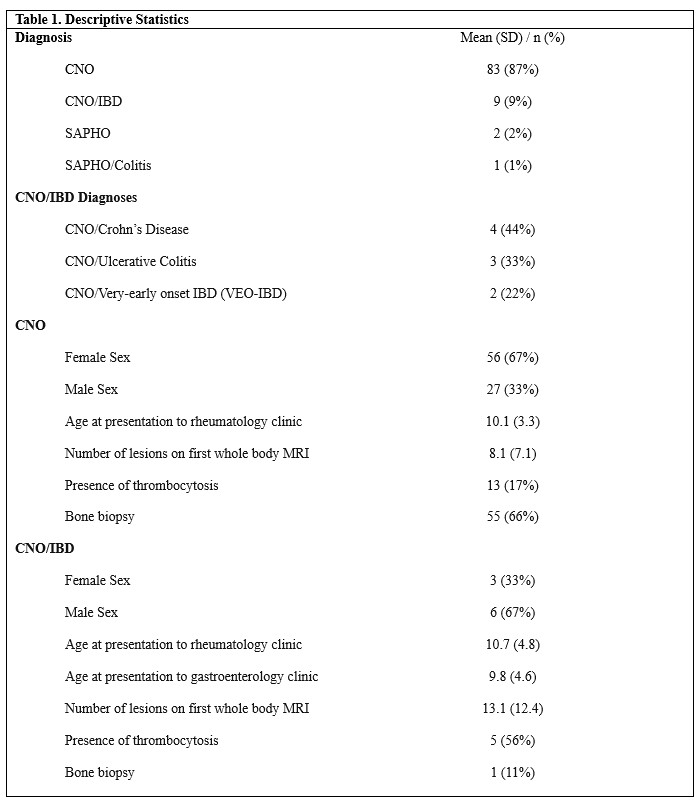
Figure 1: CNO Lesion Distribution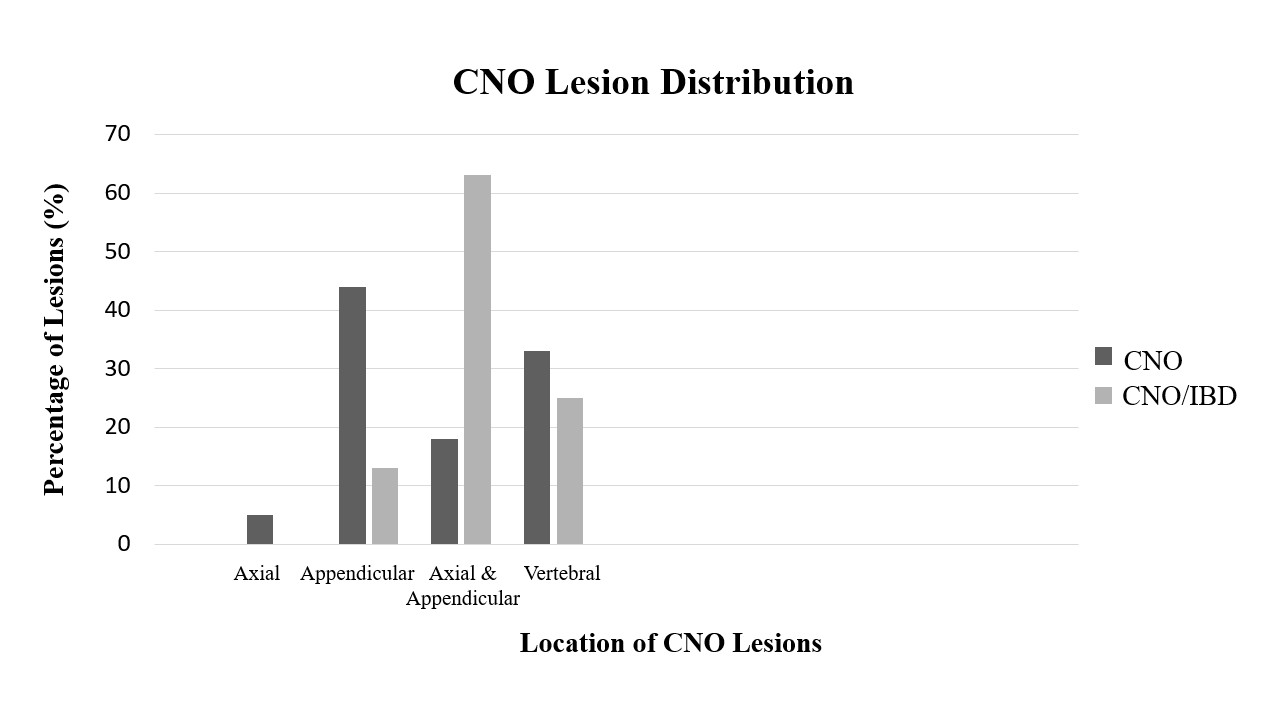
To cite this abstract in AMA style:
Wolfe M, Schildt E, Baptiste S, Nolan B. Clinical Characteristics and Diagnostic Predictors of Inflammatory Bowel Disease in Patients with Chronic Nonbacterial Osteomyelitis – A Single Center Retrospective Analysis [abstract]. Arthritis Rheumatol. 2026; 78 (suppl 3). https://acrabstracts.org/abstract/clinical-characteristics-and-diagnostic-predictors-of-inflammatory-bowel-disease-in-patients-with-chronic-nonbacterial-osteomyelitis-a-single-center-retrospective-analysis/. Accessed .« Back to 2026 Pediatric Rheumatology Symposium
ACR Meeting Abstracts - https://acrabstracts.org/abstract/clinical-characteristics-and-diagnostic-predictors-of-inflammatory-bowel-disease-in-patients-with-chronic-nonbacterial-osteomyelitis-a-single-center-retrospective-analysis/