Session Information
Date: Tuesday, November 10, 2015
Title: Vasculitis Poster III
Session Type: ACR Poster Session C
Session Time: 9:00AM-11:00AM
Childhood Takayasu
Arteritis – A Single Center Experience
Background/Purpose: Takayasu Arteritis is
a large vessel vasculitis that rarely affects
children. Data on childhood TA (cTA) are scarce.
Methods: A single-center retrospective review of all consecutive
patients fulfilling the EULAR/PRINTO/PReS criteria for
cTA between 1986 and 2015 was performed. Clinical,
laboratory and imaging features at presentation, treatment and flares (new
symptoms and/or increased inflammatory markers necessitating therapy escalation
or new angiographic lesions after 2 months of inactive disease) were captured. Disease activity was retrospectively assessed by Paediatric Vasculitis Activity Score (PVAS), damage by
Paediatric Vasculitis Damage Index (VDI). Active disease
was defined as PVAS>1 and/or increased inflammatory markers not explained by
other causes or active disease on imaging (new lesions, evidence of vessel wall
inflammation); inactive disease was defined as a PVAS=0 and normal inflammatory
markers or inactive disease on imaging. Outcome measurements included death,
disease activity and VDI at last follow-up.
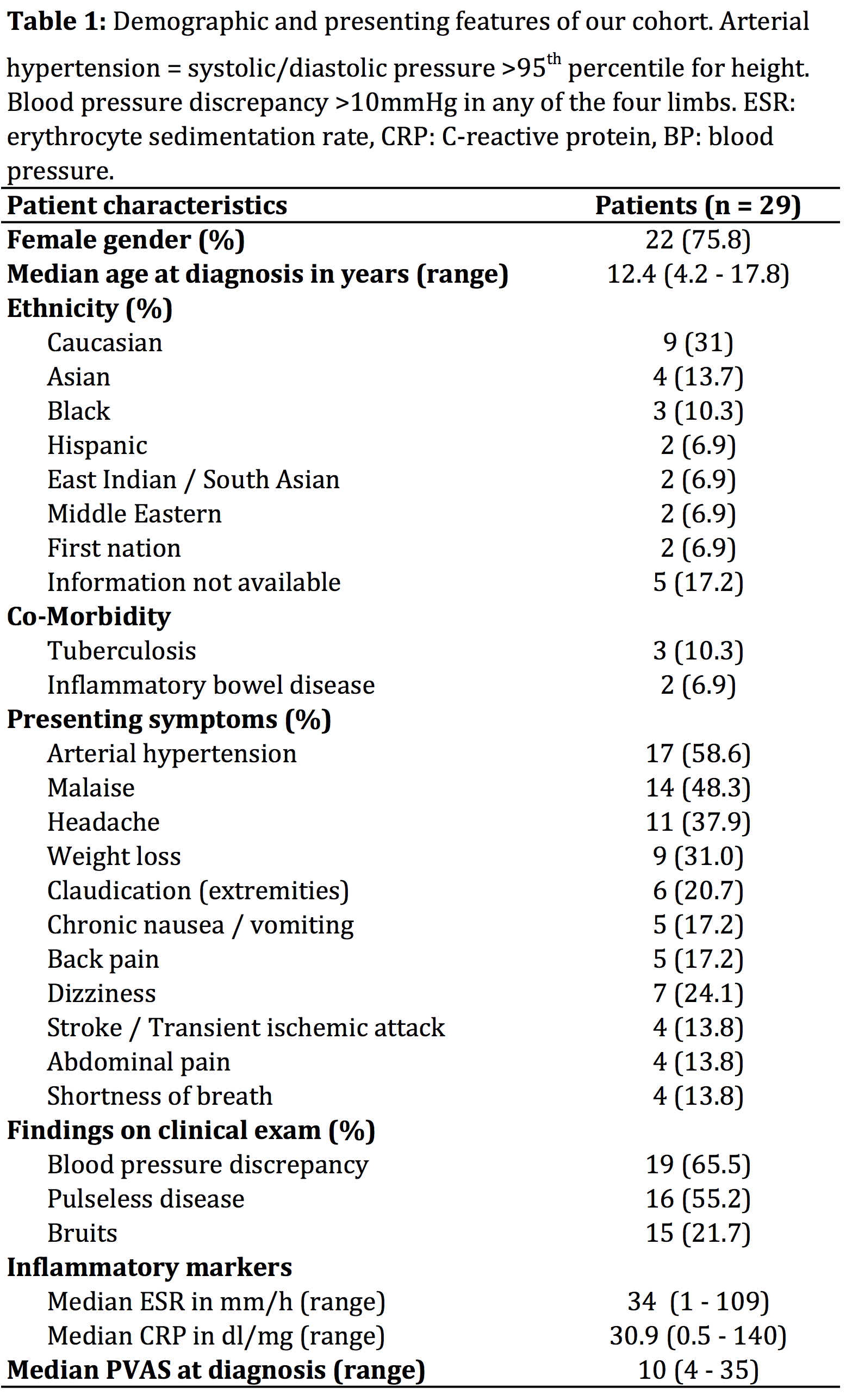
Results: Twenty-nine patients were identified; an
overview and presenting features are shown in Table 1. Most frequently involved
vessels were the abdominal aorta (86%), the renal (66%) and carotid arteries
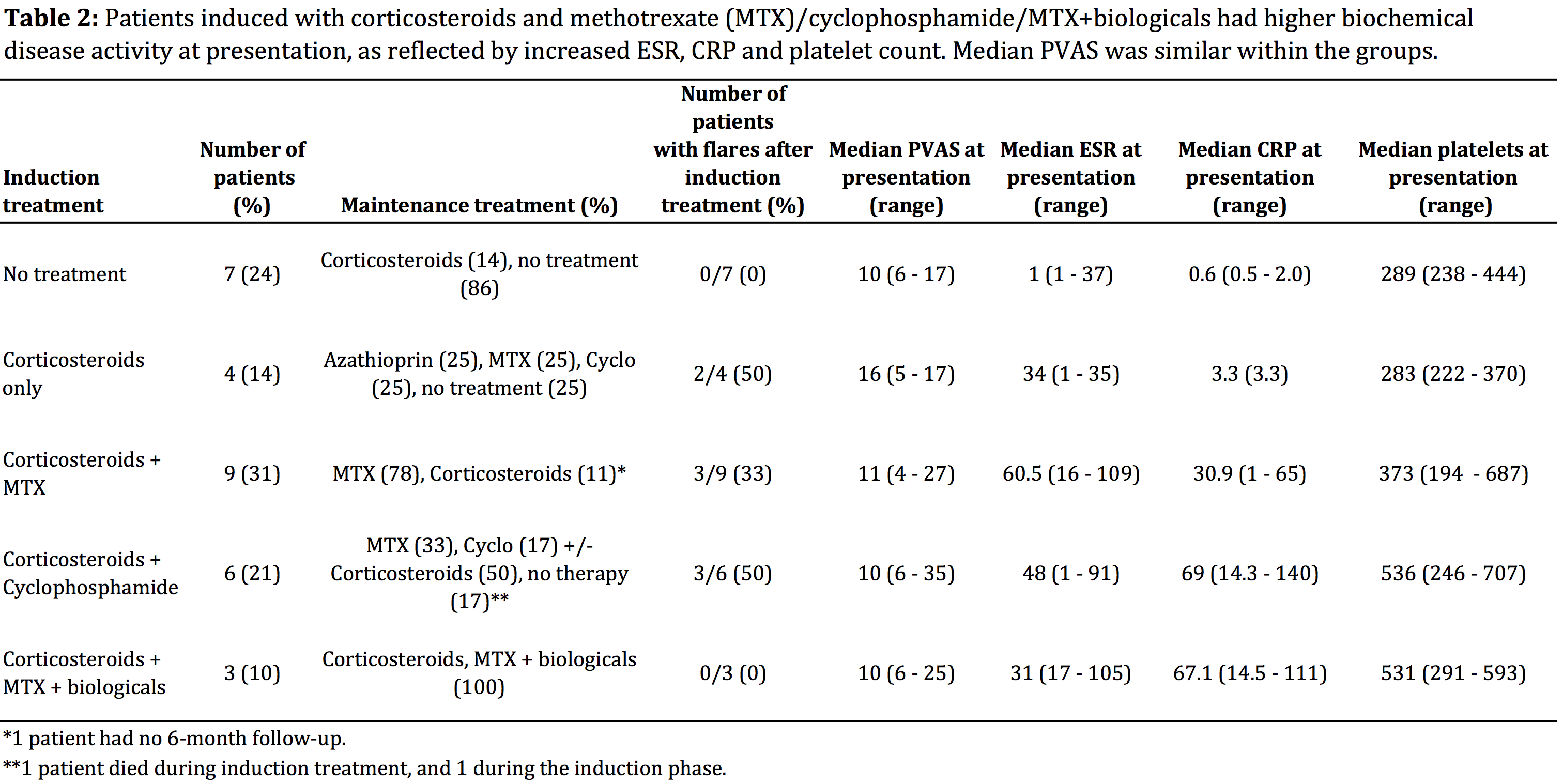
(55%). Data on induction treatment are presented in Table 2. Seven patients
were considered in a non-inflammatory disease status at diagnosis and therefore
not treated. Overall flare rate was 28%. Patients flared after a median of 12.5
months after diagnosis (range 9–73.7 months). Follow-up data were
available for 27 patients with a median follow-up time of 2.1 years (range 0.2–11.7). At last follow-up
median VDI was 4 (range 2–7); 48% of patients had active disease and 17%
inactive disease while on treatment. Another 21% had inactive disease without
treatment. Two children died within the first 6 months of diagnosis (mortality
rate 7%).
Conclusion: In this cTA cohort mortality in early disease phase and
relapse rate after induction treatment were high. At
last follow-up half of the children had active disease. We observed a discrepancy
between clinical (PVAS) and biochemical measures of disease activity, which has
to be considered regarding treatment management.
To cite this abstract in AMA style:
Aeschlimann FA, Benseler S, Laxer R, Hebert D, Sheik S, Yeung RSM. Childhood Takayasu Arteritis. a Single Center Experience [abstract]. Arthritis Rheumatol. 2015; 67 (suppl 10). https://acrabstracts.org/abstract/childhood-takayasu-arteritis-a-single-center-experience/. Accessed .« Back to 2015 ACR/ARHP Annual Meeting
ACR Meeting Abstracts - https://acrabstracts.org/abstract/childhood-takayasu-arteritis-a-single-center-experience/