Session Information
Session Type: Poster Session (Sunday)
Session Time: 9:00AM-11:00AM
Background/Purpose: Childhood-onset Takayasu’s Arteritis (TAK) may differ in presentation, clinical manifestations and treatment, as previously shown1. We aimed to compare the clinical manifestations, vascular involvement patterns, activity, damage and treatments used in childhood- and adult-onset TAK patients.
Methods: Patients from two cohorts of TAK from two tertiary-care centers in Turkey were retrospectively studied. Patients of the adult clinic were also classified as childhood-onset if they were diagnosed before the age of 18. Clinical presentation, angiographic data and treatment regimens were reviewed from clinical charts. The activity was determined by Indian Takayasu Clinical Activity Score (ITAS) on the first visit. Takayasu Arteritis Damage Score (TADS) and Vasculitis Damage Index (VDI) were employed to document the damage.
Results: Twenty four childhood-onset and 121 adult-onset TAK patients were included in the analysis (Table 1). In the basal visits, claudication of the arms [74 (62.2%) vs. 5 (20.8%), p< 0.001], carotidynia [19 (16%) vs. 0, p= 0.043], subclavian bruit [63 (58%) vs. 8 (35%), p= 0.044] and the loss of radial pulse [63 (57.8%) vs. 8 (34.8%), p= 0.044] were more common in adult-onset patients. In contrast, ischemic abdominal pain [5 (21%) vs. 8 (7%), p= 0.07], renal [9 (39%) vs. 15 (14%), p= 0.014] and abdominal bruits [11 (48%) vs. 9 (8%), p< 0.001] were more common in childhood-onset patients. Angiographic distribution of the involved vessels is shown in Table 2. Median ITAS score on the first visit was 15 (IQR: 10) for pediatric-onset and 13 (IQR: 6) for adult-onset cases (p=0.57). Medical treatment and surgical/interventional modalities are shown in Table 3. Median TADS score was 8 (IQR: 8) and 8 (IQR: 4) for pediatric and adult cases, respectively (p=0.91). Median VDI of the pediatric cases were slightly lower [ 4 (IQR:3) vs. 5 (IQR:3), p: 0.037]. Four of the adult patients and none of the pediatric patients died during follow-up. At least one episode of remission was achieved in 12 (50%) of pediatric cases and 91 (75%) of adults (p=0.013). Among patients who had information regarding activity status, 12 (50%) of pediatric cases, and 88 (82%) of the adults were in remission at the last visit.
Conclusion: In childhood-onset TAK, the involvement of the aorta was more common, whereas the upper extremity was relatively spared as evidenced by symptoms and imaging. Remission was harder to achieve in pediatric cases, and they were treated with more biologic agents. Although more surgeries were also required, the cumulative damage seemed similar in both groups.
References
- Sahin, S. et al. Childhood‐onset Takayasu arteritis: A 15‐year experience from a tertiary referral center. Int J Rheum Dis. 2019; 22: 132– 139.
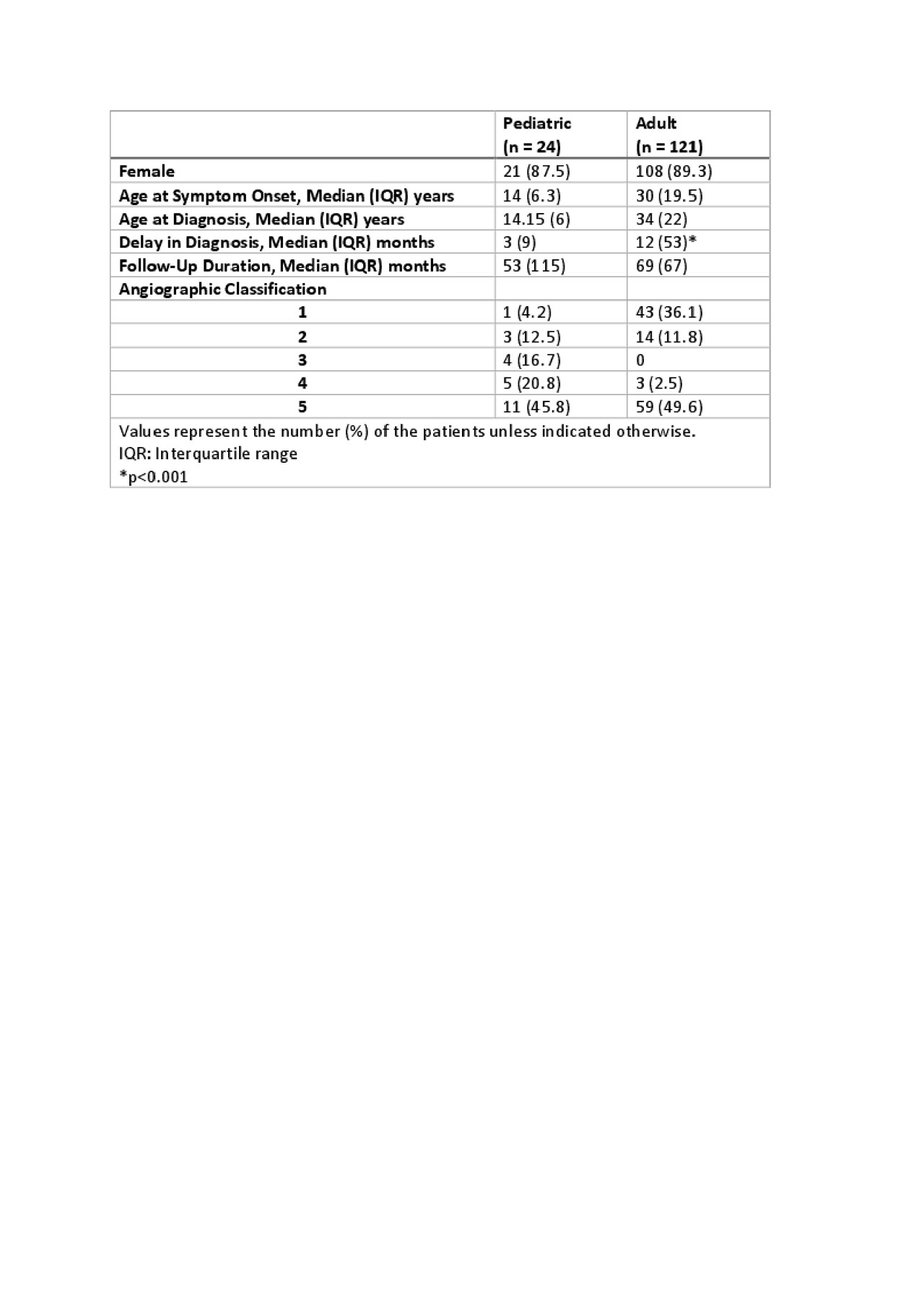
Table 1
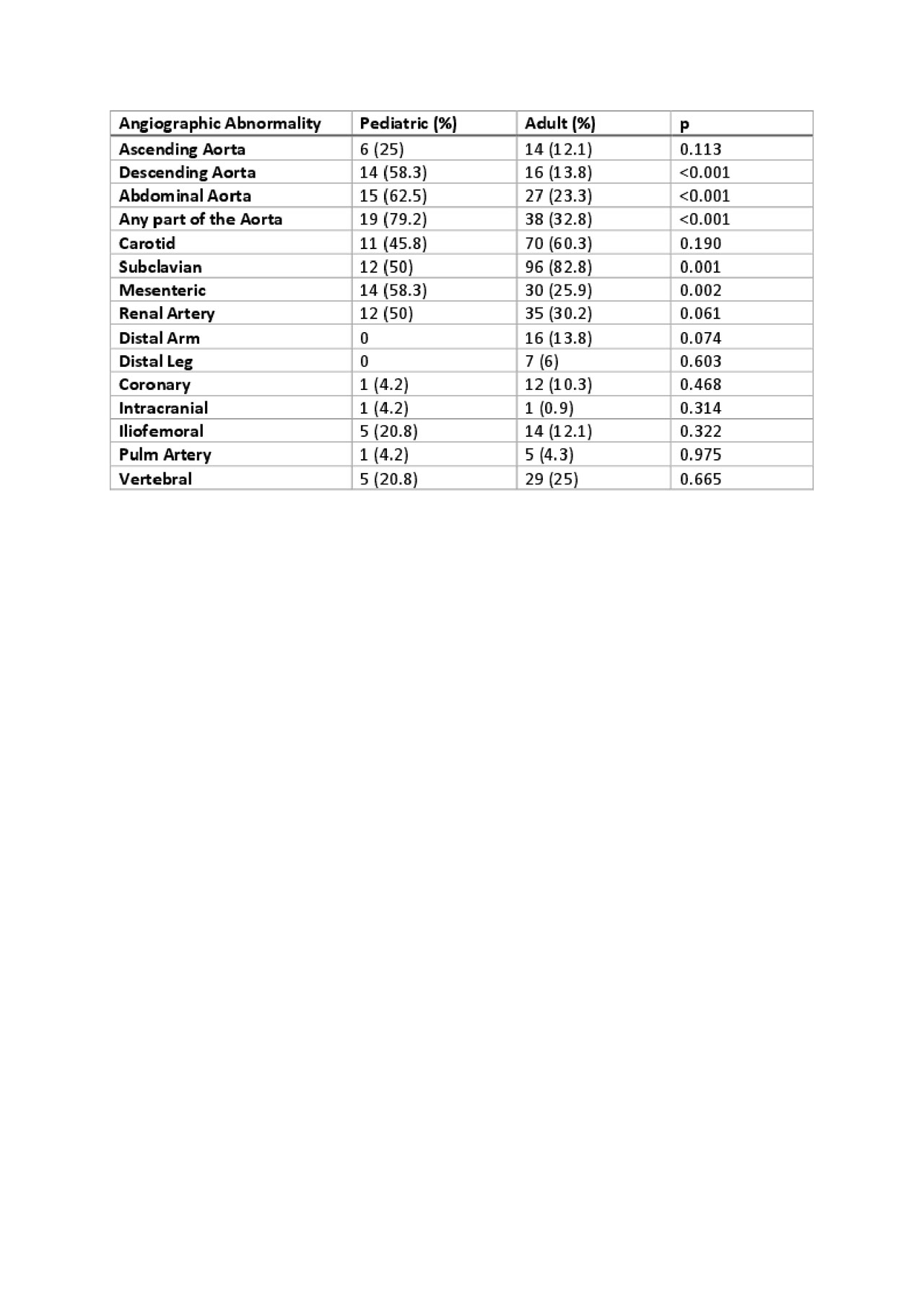
Table 2
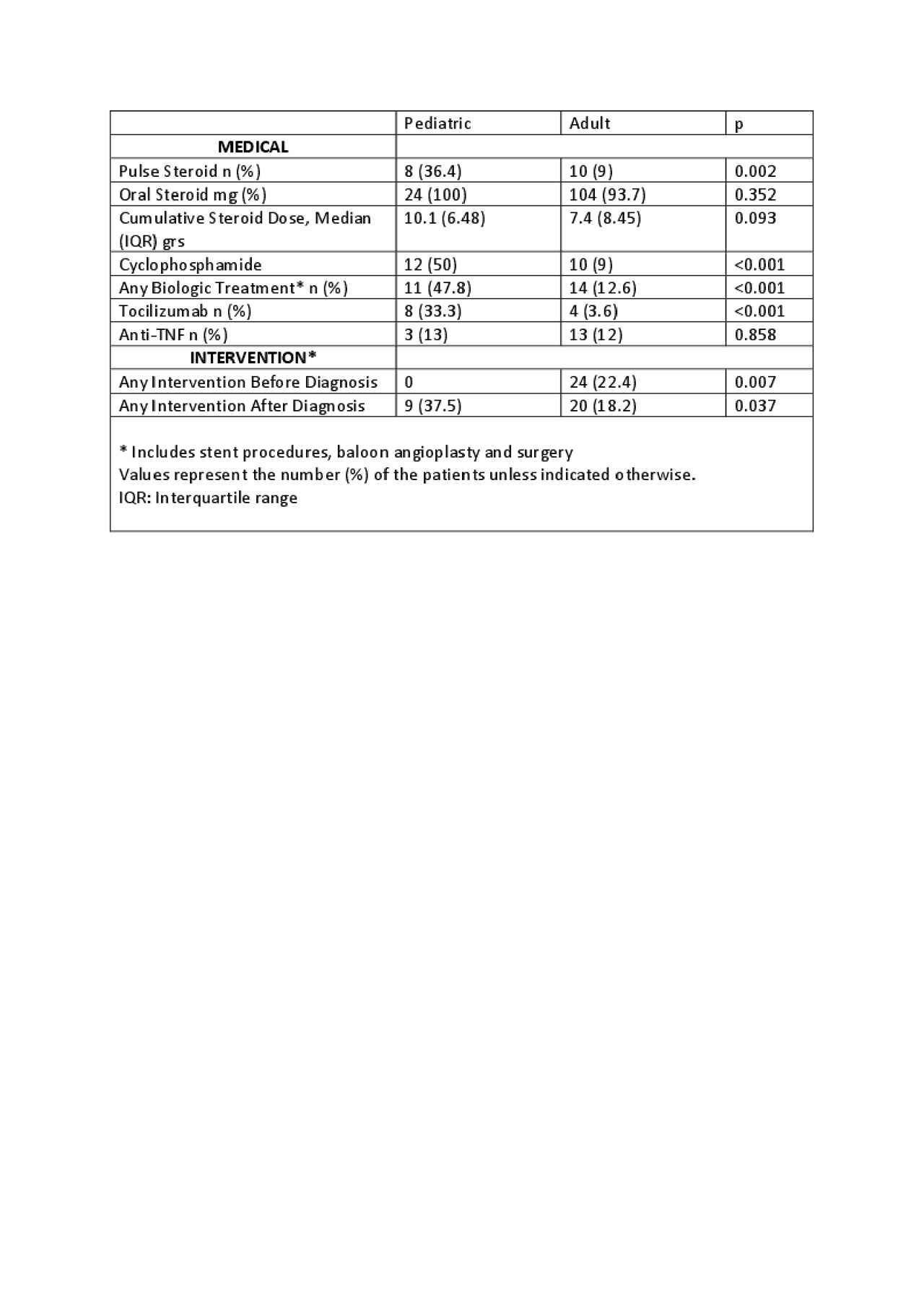
Table 3
To cite this abstract in AMA style:
Karabacak M, Kaymaz-Tahra S, Sahin S, Yıldız M, Adrovic A, Barut K, Direskeneli H, Kasapcopur O, Alibaz-Oner F. Childhood-Onset Takayasu’s Arteritis (TAK) Is Clinically More Active, However Has Similar Cumulative Damage Compared to Adult-Onset TAK [abstract]. Arthritis Rheumatol. 2019; 71 (suppl 10). https://acrabstracts.org/abstract/childhood-onset-takayasus-arteritis-tak-is-clinically-more-active-however-has-similar-cumulative-damage-compared-to-adult-onset-tak/. Accessed .« Back to 2019 ACR/ARP Annual Meeting
ACR Meeting Abstracts - https://acrabstracts.org/abstract/childhood-onset-takayasus-arteritis-tak-is-clinically-more-active-however-has-similar-cumulative-damage-compared-to-adult-onset-tak/