Session Information
Session Time: 5:00PM-6:00PM
Background/Purpose: CNS involvement in pediatric ANCA-associated vasculitis (AAV) is rare but can lead to significant neurological symptoms, including headaches, seizures, behavioral changes, and occasional cerebrovascular events. The true prevalence of CNS disease in children remains unclear. In adults, where CNS involvement affects 20–32% of cases, typical MRI findings include ischemic or hemorrhagic lesions, white matter changes, vascular narrowing, pachymeningeal thickening, and occasional pituitary abnormalities. This study characterizes the neuroradiologic features of pediatric AAV and examines their relationship to clinical presentation.
Methods: With Institutional Review Board approval, we conducted a retrospective review of pediatric AAV cases at our quaternary children’s hospital. Using SlicerDicer, we identified patients ≤18 years with granulomatosis with polyangiitis (GPA), microscopic polyangiitis (MPA), or eosinophilic GPA (EGPA) from January 2015 to August 2025. We screened for brain or spine MRI studies (standard MRI, stroke protocol, magnetic resonance angiography (MRA), or magnetic resonance venography (MRV)). Clinical and demographic data were collected, and all MRIs were interpreted by a neuroradiologist. Categorical and continuous variables were analyzed using Fisher’s Exact and Wilcoxon Rank-Sum tests.
Results: Among 70 pediatric AAV patients, 24 (34.3%) had CNS MRIs; 9 (12.9%) showed abnormalities. Demographics, antibody profiles, and clinical features were similar between those with positive and negative imaging, outlined in Table 1. Headache was the leading imaging indication. Ocular symptoms were more frequent in the negative group, while seizures were more common in the positive group, though not statistically significant. Findings included posterior reversible encephalopathy (PRES), pachymeningitis, chronic ischemic changes, gray matter heterotopia, white matter changes, and carotid narrowing. PRES, as seen in Figure 1, occurred within 6 months of AAV diagnosis, with one patient experiencing recurrence. Pachymeningitis appeared within 3 months and showed focal enhancement (Figure 2). Chronic ischemic changes were identified around 6 months, with uncertain etiology. One patient had carotid narrowing with vessel wall enhancement and cranial nerve deficits. Abnormal imaging often prompted escalation of therapy (glucocorticoids, cyclophosphamide, rituximab). None of the MRI-positive patients had persistent neurological deficits at 12-month follow-up.
Conclusion: CNS abnormalities in pediatric AAV are uncommon but clinically meaningful. Findings resemble those seen in adults, most often hypertrophic pachymeningitis, intracranial vessel narrowing, and ischemic lesions. The median 4-month interval from AAV diagnosis to abnormal imaging suggests early, uncontrolled disease that may warrant intensified or CNS-penetrating induction therapy. Neither AAV subtype, clinical features, nor imaging indications predicted MRI abnormalities, though interpretation is limited by small sample size. CNS involvement should be considered in any child with AAV who develops neurologic symptoms, particularly early in the disease course.
Table 1: Demographic and Disease Characteristics by CNS Imaging Findings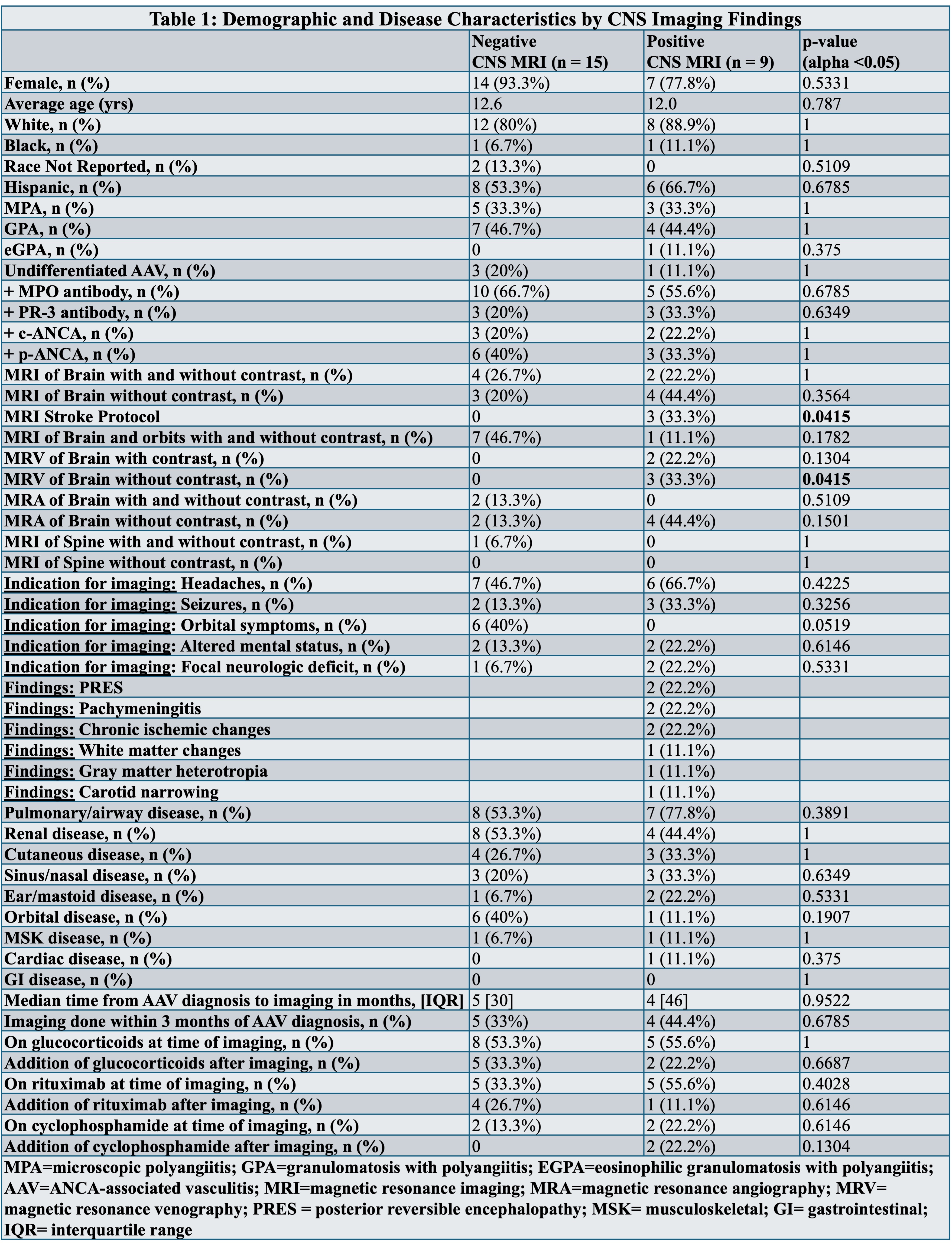
Figure 1: Posterior Reversible Encephalopathy Syndrome (PRES)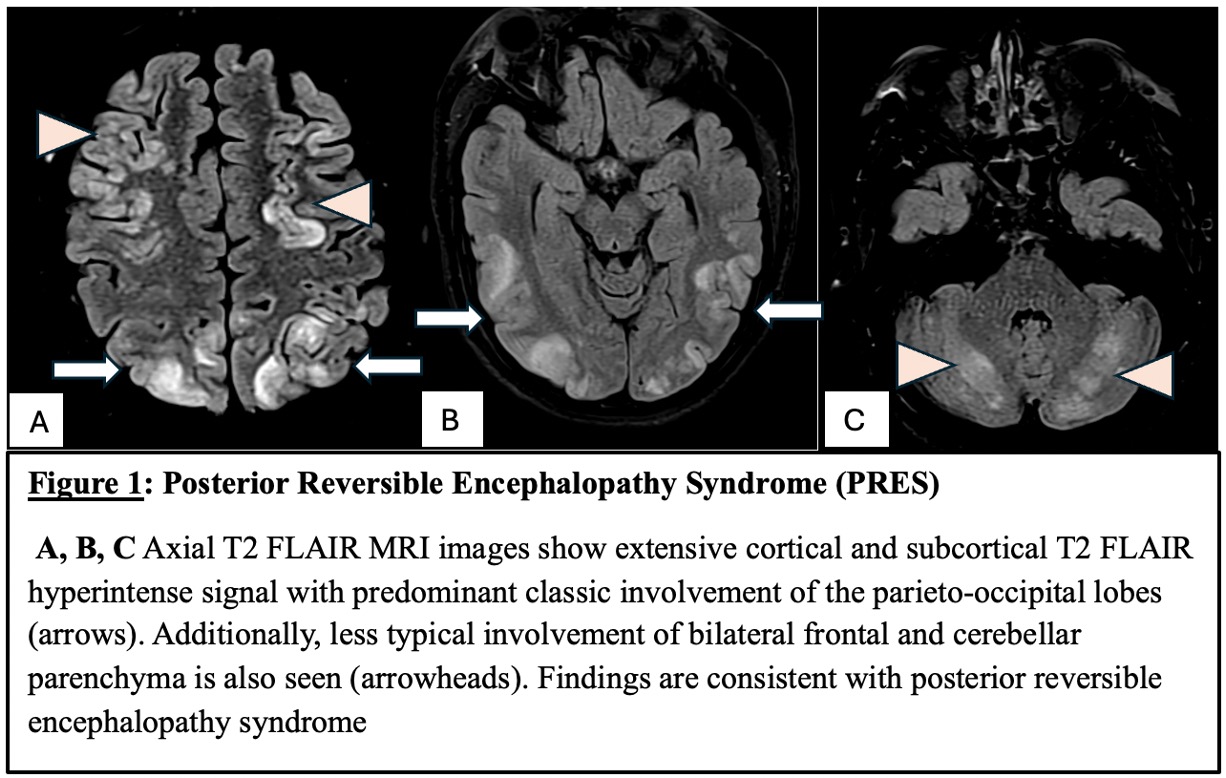 Images A, B, and C show axial T2 FLAIR MRI with extensive cortical and subcortical T2 FLAIR hyperintense signal with predominant classic involvement of the parieto-occipital lobes (arrows). Additionally, less typical involvement of bilateral frontal and cerebellar parenchyma is also seen (arrowheads). Findings are consistent with posterior reversible encephalopathy syndrome (PRES).
Images A, B, and C show axial T2 FLAIR MRI with extensive cortical and subcortical T2 FLAIR hyperintense signal with predominant classic involvement of the parieto-occipital lobes (arrows). Additionally, less typical involvement of bilateral frontal and cerebellar parenchyma is also seen (arrowheads). Findings are consistent with posterior reversible encephalopathy syndrome (PRES).
Figure 2: Pachymeningitis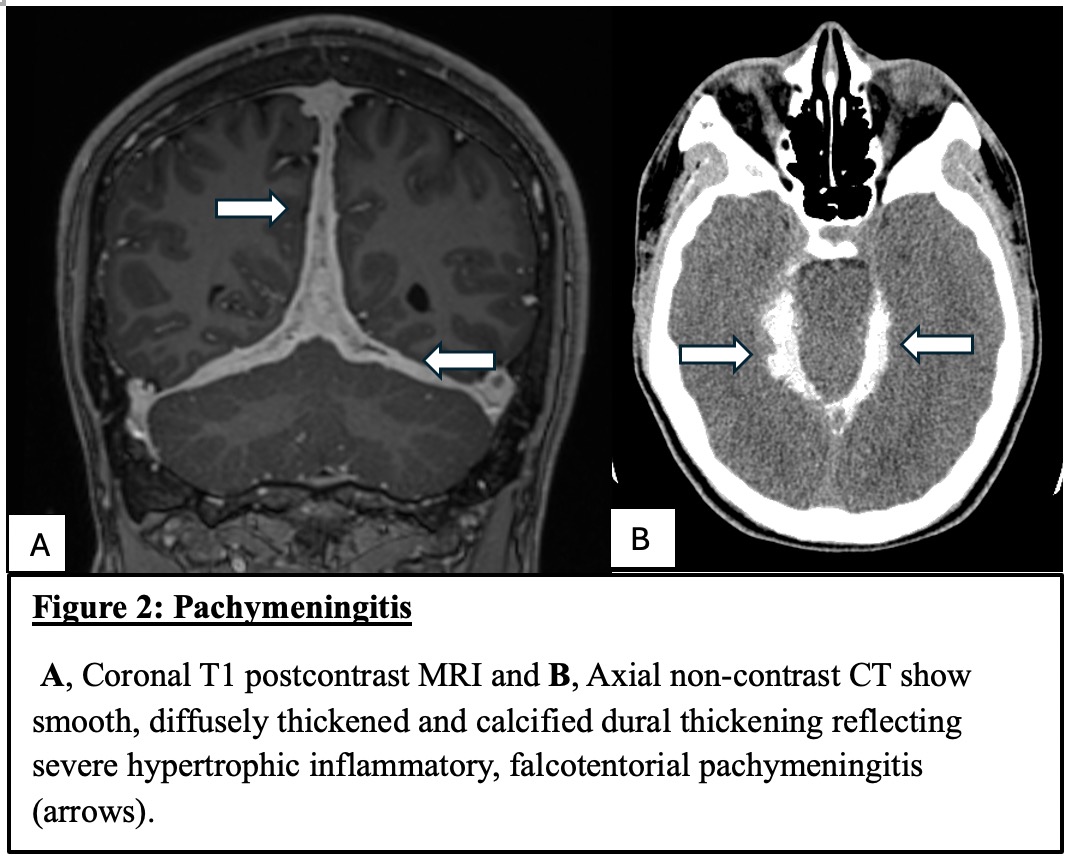 A, Coronal T1 post-contrast MRI and B, Axial non-contrast CT show smooth, diffusely thickened and calcified dural thickening reflecting severe hypertrophic inflammatory, falcotentorial pachymeningitis (arrows).
A, Coronal T1 post-contrast MRI and B, Axial non-contrast CT show smooth, diffusely thickened and calcified dural thickening reflecting severe hypertrophic inflammatory, falcotentorial pachymeningitis (arrows).
To cite this abstract in AMA style:
Gist D, Muscal E, Narayanan S, Thomas D. Characterizing CNS MRI Abnormalities in Pediatric ANCA-Associated Vasculitis [abstract]. Arthritis Rheumatol. 2026; 78 (suppl 3). https://acrabstracts.org/abstract/characterizing-cns-mri-abnormalities-in-pediatric-anca-associated-vasculitis/. Accessed .« Back to 2026 Pediatric Rheumatology Symposium
ACR Meeting Abstracts - https://acrabstracts.org/abstract/characterizing-cns-mri-abnormalities-in-pediatric-anca-associated-vasculitis/