Session Information
Date: Monday, November 18, 2024
Title: Abstracts: Vasculitis – Non-ANCA-Associated & Related Disorders II
Session Type: Abstract Session
Session Time: 3:00PM-4:30PM
Background/Purpose: The management of giant cell arteritis (GCA) has evolved with the arrival of tocilizumab (TCZ) and the use of PET/CT. In modern era, a double clinical challenge persists: to reduce relapse rate and glucocorticoids (GC) exposure. Our objective is to describe the characteristics and follow-up of patients with recent diagnosis of GCA in current care.
Methods: The NEWTON cohort is a French multicentric retrospective cohort based on data collected from GCA patients diagnosed after 2016 and who satisfied the ACR/EULAR 2022 criteria. Relapse definition was 1/ clinical symptom related to GCA and/or elevated C-reactive protein and/or worsening or new vascular lesion, in a patient previously in remission, and 2/ the need for the reinstitution or an increase in prednisone, and/or the addition of, or a change in, immunosuppressive drug (IS). Relapse characteristics, factor associated with the first relapse and therapeutic managements were analysed.
Results: We identified 211 GCA diagnosed between 2017 and 2023, with a mean (± SD) age at diagnosis of 77.2 (± 9.58) years, female predominance (n=142 ; 67.3%) and followed up for a median duration [IQR Q1 ; Q3] of 35 [19 ; 56] months. GCA relapse occurred in 109/211 (51.6%) patients with 240 relapses. The median time at first relapse was 261 [125 ; 468] days, following GCA diagnosis. At relapse, prednisone discontinuation was observed in 40/240 (16.7%), the median dose of prednisone was 6.5 [0 ; 12.5] mg daily, increased to 20 [10 ; 35] mg daily after therapeutic intensification. Relapses characteristics included clinical and biological criteria in 82/240 (34%), clinical criteria alone in 69/240 (29%), biological criteria alone in 36/240 (15%), clinical and imaging criteria in 15/240 (6%), imaging and biological criteria in 7/240 (3%) or imaging criteria alone in 7/240 (3%). Therapeutic intensifications following relapse included reinstitution or increase in GC alone in 43%, GC and IS intensification in 32%, and addition of IS alone in 25%. During the disease course, 64/211 (30%) patients received TCZ either from diagnosis in 16/64 (25%), either at relapse in 48/64 (75%). Subcutaneous TCZ was used in 41/64 (64%) and intravenous TCZ in 23/64 (36%). Among them, 31 (48%) patients discontinued TCZ, 19 (30%) because of remission while 12 (18%) patients discontinued because of TCZ adverse events. After TCZ discontinuation with a median follow-up of 17.5 [11.5 ; 31] months, 11/31 (35.5%) patients relapsed in a median time of 133 [90 ; 303.5] days. Twenty (64.5%) patients did not relapse after TCZ cessation with a median follow-up of 511 [153.3 ; 611.5] days.
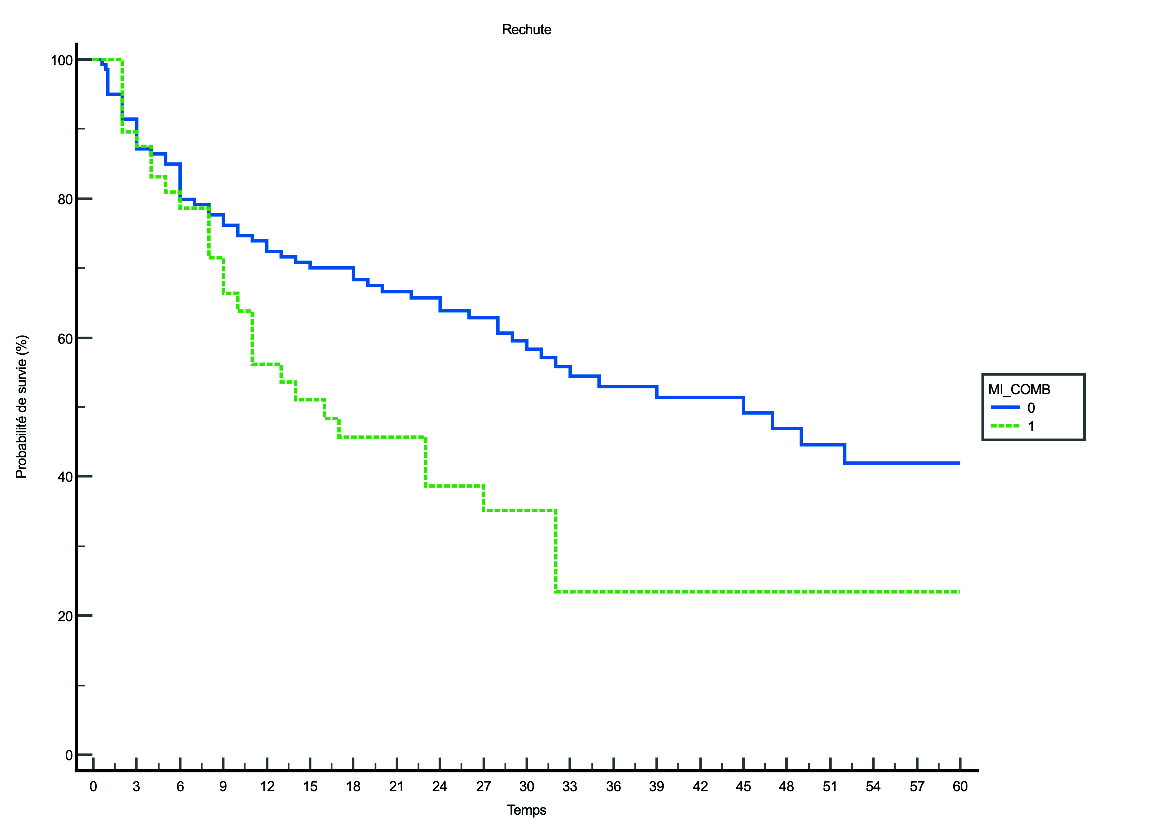
Multivariable Cox regression model, including clinical symptom and age at GCA diagnosis, gender, vascular lesion in different topography related to GCA as covariates, showed that only limb arteries involvement (HR 1.9 [1.23-2.98], P< 0.01) at diagnosis was associated with GCA relapse.
Conclusion: Relapses occur mainly during the year following diagnosis, despite GC are not discontinued. The use of TCZ concerns a third of GCA recently diagnosed, however more than one third relapsed after TCZ cessation. Limb arteries involvement at GCA diagnosis is a predictor of relapse.
To cite this abstract in AMA style:
Peyrac G, Lomba Goncalves N, Kante A, Cacoub P, Sacré K, Saadoun D, Papo T, Alexandra J, Pagis V, Bourdin V, Richette P, Vanjak A, Latourte A, Elessa D, Bigot W, burlacu R, Champion K, Amador Borrero B, Lopes A, Depond A, Reiner P, Adle-Biassette H, Couturier A, Bonnin P, Boutigny A, Paycha F, Couvelard A, Régent A, Chaigne B, Nguyen Y, lefort A, Bory O, Aslangul E, mouly s, Sène D, Tran V, Comarmond C. Characteristics of Relapse and Therapeutic Management in Giant Cell Arteritis in Modern Era, NEWTON Study [abstract]. Arthritis Rheumatol. 2024; 76 (suppl 9). https://acrabstracts.org/abstract/characteristics-of-relapse-and-therapeutic-management-in-giant-cell-arteritis-in-modern-era-newton-study/. Accessed .« Back to ACR Convergence 2024
ACR Meeting Abstracts - https://acrabstracts.org/abstract/characteristics-of-relapse-and-therapeutic-management-in-giant-cell-arteritis-in-modern-era-newton-study/