Session Information
Session Type: Poster Session D
Session Time: 1:00PM-3:00PM
Background/Purpose: Arthritis is one of the most common manifestations in an FMF attack. It is usually in the form of acute mono- or oligoarthritis of the large joints of the lower extremities. While acute attacks of arthritis usually subside without causing permanent deformity, the long-lasting form of chronic arthritis can last for months or even years and result in permanent deformity. In this study, we described the joint involvement pattern in FMF patients.
Methods: Our FMF cohort consisted of 2350 patients who were diagnosed according to Tel Hashomer criteria and followed up in our center. Their records were retrospectively scanned through the files and hospital system to detect patients with joint involvement. The prevalence, demographic information, genetic test results, clinical features, joint involvement, treatments and responses, and family history of patients with joint involvement were recorded.
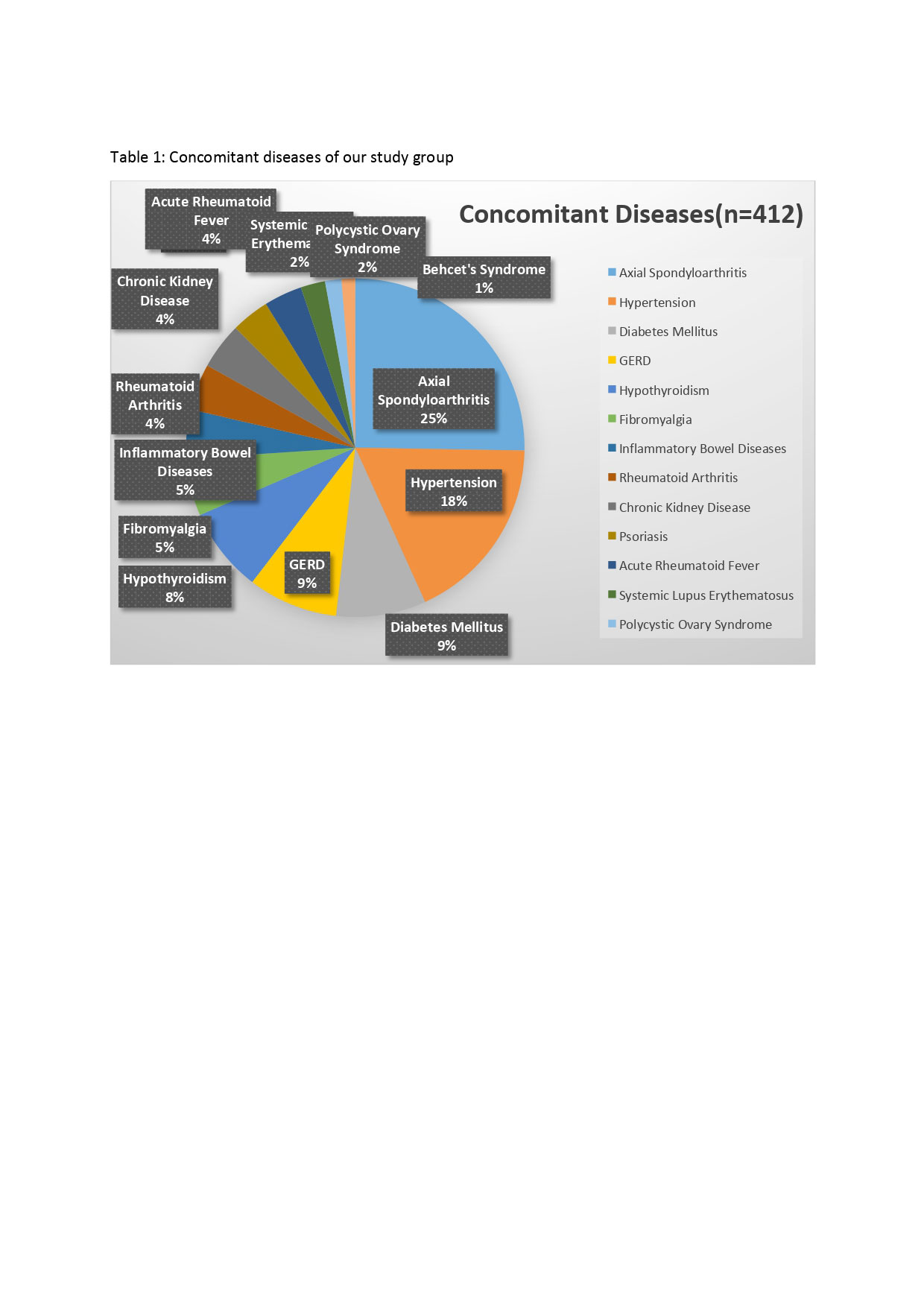
Results: 954 patients out of 2350 FMF patients had arthralgia or arthritis (40%). The male/female ratio was 0.5 (316 males, 638 females). The number of patients who underwent genetic testing was 787 (82%), and 702 (89%) of these patients had MEFV gene mutations. The most common pathogenic mutation was M694V mutation with a rate of %65. Concomitant diseases and their frequencies are shown in Table 1, with the most common one being axial spondyloarthritis with a rate of 27%. Arthritis or arthralgia was present in the first attack in 73% (n=695). 182 patients (19%) only had arthritis during the first attack. The duration of FMF attack was between 24-96 hours in 77% (n=837) of the patients, and the duration was longer than 96 hours in 23% (n=116). The most common finding accompanying the attacks was exercise-related leg pain. Family history was present in 61% (n=580). 73% of the patients (n=696) had ankle involvement and 51% (n=492) had knee involvement. The incidence of sacroiliitis was 14% (n=142). 91% of the patients had mono- or oligoarthritis (58% monoarthritis, 34% oligoarthritis). Asymmetric involvement was detected in 77% of the patients. Red arthritis was present in %73 of the patients. HLA-B27 was examined in 185 patients, 24 of them were positive (12%). 43% of the patients had treatment changes due to arthritis. Colchicine dose increases or preparation changes were needed in 32% of these patients. NSAIDs were started in 21%, corticosteroids in 15%, DMARDs in 12%, anti-TNF in 10%, and anti-IL-1 in 8% of the patients. The mean daily dose of colchicine was 1.56 ± 0.5 mg. Unresponsiveness to colchicine was found in 21% (n=122).
Conclusion: FMF diagnosis should be considered in people with red mono-oligoarthritis in the large joints of the lower extremities. One of the most important features of joint involvement in FMF patients is its short duration. The accompanying effort-related leg pain is a supportive finding for FMF. In FMF patients with arthritis, the required colchicine dose in the treatment and the rate of colchicine unresponsiveness were higher than the average FMF population. The incidence of spondyloarthropathy was increased in FMF patients. FMF should be in the differential diagnoses of the patients with inflammatory low back pain.
To cite this abstract in AMA style:
Ayla A, Yenigun S, baspinar s, Yuzbasioglu M, Alkan A, Durucan I, kirman m, polat b, ergun s, Ugurlu S, Ozdogan H. Characteristics of Arthritis in Familial Mediterranean Fever Patients [abstract]. Arthritis Rheumatol. 2022; 74 (suppl 9). https://acrabstracts.org/abstract/characteristics-of-arthritis-in-familial-mediterranean-fever-patients/. Accessed .« Back to ACR Convergence 2022
ACR Meeting Abstracts - https://acrabstracts.org/abstract/characteristics-of-arthritis-in-familial-mediterranean-fever-patients/