Session Information
Session Type: ACR Poster Session A
Session Time: 9:00AM-11:00AM
Background/Purpose: Prior studies observed better disease control, quality of life, and physical function among patients with rheumatoid arthritis (RA) who drink alcohol. These studies may suffer from reverse causality due to discontinuation of use over time among those with poor health. We assessed factors associated with changes in alcohol use over time and the effects of discontinuation on disease activity and mortality in a large RA registry.
Methods: RA participants in FORWARD, the National Databank for Rheumatic Diseases, were asked about alcohol use on semi-annual surveys (any v. none). Our disease activity measure was the Patient Activity Scale 2 (PAS2). Logistic regression models with generalized estimating equations assessed associations between patient factors and alcohol use at the time of the next questionnaire among those reporting current regular alcohol intake. Multivariable logistic regression and Cox proportional hazards models illustrated survival of alcohol use over time by disease activity categories and assessed the risk of discontinuation of alcohol use on subsequent worsening of disease activity (>0.5 standard deviation change) and mortality.
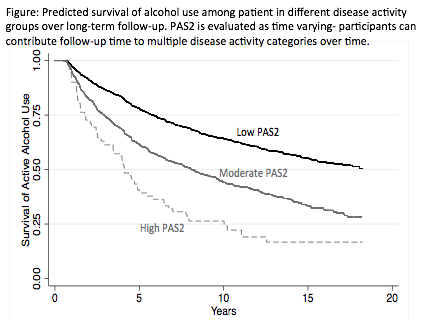
Results: In 121,280 observations (16,722 unique patients), alcohol users had lower PAS2 [β: -0.18 (-0.21, -0.15) p<0.001]. Discontinuation of alcohol was common among drinkers (8.2% of observations). Higher disease activity was associated with future discontinuation of alcohol (Table, Figure). This was explained by other factors associated with discontinuation: older age, female sex, non-white race, obesity, comorbidity, work disability, low educational level and income, and poor physical/mental quality of life. Recent discontinuation (in prior 6 month interval) was not independently associated with a subsequent increase in PAS2 over the subsequent 6 months after adjustment [OR 1.03 (0.94, 1.13) p=0.58]. Discontinuation was associated with a greater risk of death [HR 1.58 (1.25, 2.00) p<0.001], but not independently of the above factors [HR 1.13 (0.86, 1.47) p=0.36]. Sensitivity analyses limited only to moderate alcohol use were similar.
Conclusion: Higher disease activity, disability, comorbidity, and poor quality of life are associated with discontinuation of alcohol use in RA. Discontinuation of alcohol is not independently associated with worsening disease activity or greater mortality. These observations highlight a need to ensure that a behavioral exposure temporally precedes the outcome in epidemiologic studies and calls into question previously described benefits of alcohol consumption in RA.
|
Table: Associations between disease activity and discontinuation of alcohol use. |
||||
|
Model 1 Odds of Discontinuation (N=7,937; Obs=52,345)
|
Model 2 Odds of Discontinuation (N=7,817; Obs=51,073)
|
|||
|
OR (95% CI) |
p |
OR (95% CI)
|
p |
|
|
Age <50
|
Reference |
Reference |
||
|
Age 50-60 |
1.02 (0.92, 1.13) |
0.71 |
1.01 (0.90, 1.12) |
0.90 |
|
Age 60-70 |
1.08 (0.97, 1.20) |
0.18 |
1.04 (0.93, 1.16) |
0.13 |
|
Age 70-80 |
1.22 (1.09, 1.37) |
0.001 |
1.12 (0.98, 1.27) |
0.002 |
|
Age >80
|
1.54 (1.32, 1.80) |
<0.001 |
1.27 (1.08, 1.51) |
0.005 |
|
Male |
0.69 (0.61, 0.77) |
<0.001 |
0.72 (0.64, 0.81) |
<0.001 |
|
White |
0.69 (0.58, 0.82) |
<0.001 |
0.73 (0.62, 0.87) |
<0.001 |
|
BMI |
||||
|
Low
|
1.04 (0.73, 1.49) |
0.81 |
1.03 (0.71, 1.50) |
0.86 |
|
Normal
|
Reference |
Reference |
||
|
Overweight
|
1.10 (0.98, 1.23) |
0.16 |
1.04 (0.93, 1.17) |
0.47 |
|
Obese
|
1.57 (1.41, 1.75) |
<0.001 |
1.37 (1.22, 1.54) |
<0.001 |
|
Methotrexate |
1.04 (0.97, 1.12) |
0.28 |
1.05 (0.97, 1.13) |
0.21 |
|
Prednisone |
1.10 (1.03, 1.19) |
0.008 |
1.06 (0.98, 1.14) |
0.16 |
|
Any Biologic |
0.92 (0.86, 0.99) |
0.02 |
0.94 (0.87, 1.01) |
0.08 |
|
PAS2 |
||||
|
Remission
|
Reference |
Reference |
||
|
Low
|
1.36 (1.27, 1.44) |
<0.001 |
1.07 (1.00, 1.15) |
0.06 |
|
Mod-High
|
1.85 (1.37, 2.51) |
<0.001 |
1.22 (0.90, 1.66) |
0.19 |
|
Work Disability |
— |
— |
1.18 (1.06, 1.32) |
0.003 |
|
RDCI |
— |
— |
1.02 (1.00, 1.04) |
0.02 |
|
Liver Disease |
— |
— |
1.23 (0.99, 1.53) |
0.07 |
|
Physical QOL |
— |
— |
0.99 (0.98, 0.99) |
<0.001 |
|
Mental QOL |
— |
— |
0.99 (0.99,1.00) |
0.001 |
|
Education ³16 yrs
|
— |
— |
0.84 (0.76, 0.93) |
0.001 |
|
Income (Ref 0-25K) |
— |
— |
Reference |
— |
|
35-55K
|
— |
— |
0.84 (0.77, 0.92) |
<0.001 |
|
65-150K
|
— |
— |
0.72 (0.65, 0.79) |
<0.001 |
To cite this abstract in AMA style:
Baker J, Sayles H, England BR, Mikuls TR, Michaud K. Changes in Alcohol Use in Patients with Rheumatoid Arthritis: Associations with Disease Activity, Health Status, and Mortality [abstract]. Arthritis Rheumatol. 2018; 70 (suppl 9). https://acrabstracts.org/abstract/changes-in-alcohol-use-in-patients-with-rheumatoid-arthritis-associations-with-disease-activity-health-status-and-mortality/. Accessed .« Back to 2018 ACR/ARHP Annual Meeting
ACR Meeting Abstracts - https://acrabstracts.org/abstract/changes-in-alcohol-use-in-patients-with-rheumatoid-arthritis-associations-with-disease-activity-health-status-and-mortality/