Session Information
Date: Monday, November 13, 2023
Title: (1124–1154) Miscellaneous Rheumatic & Inflammatory Diseases Poster II
Session Type: Poster Session B
Session Time: 9:00AM-11:00AM
Background/Purpose: The newly described VEXAS syndrome is a very heterogenous disease with rheumatologic and hematologic manifestations, caused by somatic mutations affecting UBA1 gene, that still requires a precise definition. This report aims to address diagnostic challenges such as delays in diagnosis, misdiagnosis, and the clinical associations observed between specific genetic mutations and VEXAS patients (VP).
Methods: A comprehensive survey covering the whole country, which included 126 Spanish hospitals with rheumatologic units, was performed to identify all the VP observed in those units. VP were defined as compatible clinical picture plus characteristic BMB and/or confirmed genetic UBA1 gene mutations. Demographic and clinical data, along with the timing of initial symptoms, initial and final diagnoses, and specific gene mutations identified in each case, were gathered from medical records. Descriptive analyses were conducted employing standard tests.
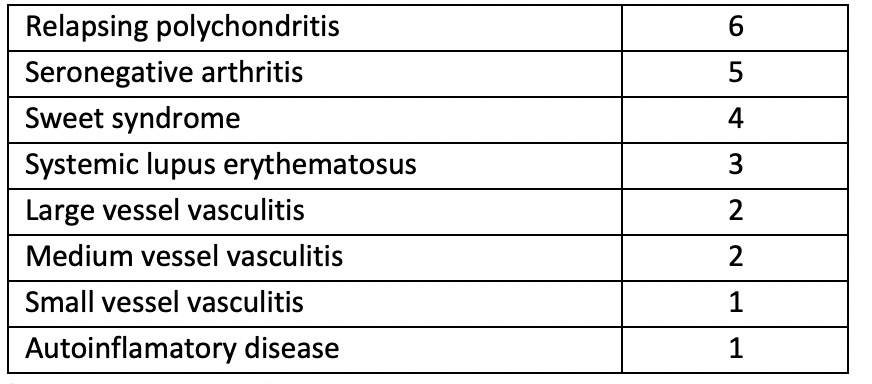
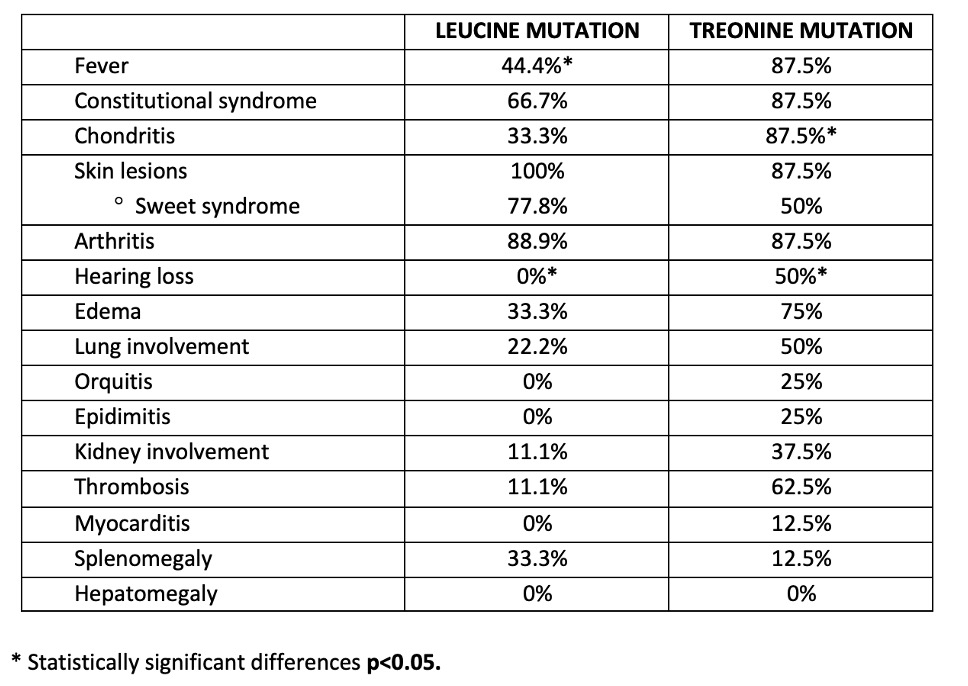
Results: Twenty-eight VP were identified. Mean age at onset of symptoms was 65.46 (±SD 9.44/range 40-78) years of age, while mean age at final diagnostic was 70.96 (±SD 8.92/range 46-83) years of age.Median diagnostic delay was 65.34 (±SD 41.73) months and median time from first symptom appearance to Rheumatology referral was 26.29 (±SD 41.73) months. Diagnoses prior to VEXAS syndrome are summarised in Table 1. Twenty-six (92.85%) patients underwent bone marrow biopsy; presence of at least 1 cytoplasmic vacuole was described in 23 cases. Genetic tests were performed in 23 (82.14%) patients. Within our cohort, among the three primary causative variants, 10 patients exhibited an M41L mutation, 8 patients had an M41T mutation, and 3 patients presented an M41V mutation. One patient presented a novel variation affecting c.209T >A, causing a leucine to histidine change, this alteration has not been previously described in other studies to our knowledge at the time of this publication. Finally, data regarding specific mutation was missed in a case. The mutation causing a change to leucine was associated with a phenotype more limited to the skin and joints, with absence of other manifestations as chondritis, hearing loss, or pulmonary involvement. In contrast, the threonine mutation was associated with a broader repertoire of clinical manifestations. Most of these associations were numerical rather than statistically significant (with the exceptions of negative association between hearing loss and leucine mutation and the positive one of chondritis with threonine) due to sample size limitations (Table 2). Finally, out of the 3 (10.71%) patients who died, 2 had leucine and 1 threonine mutations.
Conclusion: The VEXAS syndrome presents a significant delay in its detection as it is quite common its misdiagnosis for other multisystemic entities. Leucine mutation seems to be more associated with cutaneous and articular involvement, whereas the threonine mutation is more associated with chondritis and a more multi-organ clinical picture. These associations need further clarification through larger cohorts, which should also investigate the role of the novel mutation (c.209T >A: p.L70H) identified in this particular cohort.
To cite this abstract in AMA style:
García Escudero P, López i Gómez M, López Maraver M, VELA P, Rodríguez Laguna M, Merino c, Orenes Vera A, García Belando C, Dios Santos D, Miranda Filloy J, Toyos Sáenz de Miera F, Garcia Dorta A, Vázquez I, Hernández Beriain J, DIEZ ALVAREZ M, Ibáñez Martínez M, Frade Sosa B, Font Urgelles J, Salles Lizarzaburu M, Riera Alonso E, Trallero Araguás E, Magallanes López B, Belzunegui Otano J, de Miguel Sánchez C, Ortiz de Zárate Caballero Z, Calvo Alén J. Challenges in Diagnosing VEXAS Syndrome: Delayed Diagnosis, Misdiagnosis, and Associations with Specific Gene Mutations [abstract]. Arthritis Rheumatol. 2023; 75 (suppl 9). https://acrabstracts.org/abstract/challenges-in-diagnosing-vexas-syndrome-delayed-diagnosis-misdiagnosis-and-associations-with-specific-gene-mutations/. Accessed .« Back to ACR Convergence 2023
ACR Meeting Abstracts - https://acrabstracts.org/abstract/challenges-in-diagnosing-vexas-syndrome-delayed-diagnosis-misdiagnosis-and-associations-with-specific-gene-mutations/